 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Blindness Caused by Diabetes -- Massachusetts, 1987-1994Diabetes, the leading cause of new blindness among U.S. adults aged 20-74 years, accounts for approximately 8% of cases of legal blindness and 12% of all new cases of blindness in the United States each year (1). One of the national health objectives for the year 2000 is to decrease by 50% the incidence of blindness caused by diabetes (objective 17.10) (2). However, surveillance for blindness among persons with diabetes has not been conducted nationally, and national prevalence estimates of blindness caused by diabetes have been based on state data from the register of the Massachusetts Commission for the Blind (MCB). To characterize recent trends, data on legal blindness caused by diabetes among adults with diabetes in Massachusetts were examined for 1987-1994. This report summarizes the results of that analysis, which indicate that in Massachusetts, the overall incidence and prevalence of legal blindness caused by diabetes did not decrease, despite the availability of methods to prevent vision loss. Massachusetts General Law (Chapter 6, Section 136) requires institutions, physicians, ophthalmologists, and optometrists to report all persons with legal blindness to MCB within 30 days of diagnosis. Legal blindness is defined as a corrected visual acuity of 20/200 or worse in the better eye or a field of vision of less than or equal to 10 degrees (3). Data collected by MCB include best corrected visual acuity, field of vision, and cause of blindness, including site or type of lesion (e.g., glaucoma, cataract, or retinopathy) and etiology (e.g., diabetes). Causes are coded according to the National Society for the Prevention of Blindness standard classification manual * (3). Persons who had died or moved out of state were removed from the registry in 1987, 1991, and 1994. For calculating the annual incidence and prevalence of blindness caused by diabetes among persons with diabetes, the denominator was the estimated number of persons with diabetes in Massachusetts; this number was derived from intercensal population estimates for the state and national estimates of the prevalence of diagnosed diabetes in the National Health Interview Survey **. For 1993 and 1994, intercensal population estimates for 1992 were used. For 1994, estimates of the prevalence of diagnosed diabetes for 1993 were used. Rates for men, women, and both sexes combined were age-adjusted to the estimated population of persons with diabetes in Massachusetts in 1987. During 1987-1994, blindness caused by diabetes was reported for 2990 persons (annual mean: 374, range: 340-397); 60% were aged greater than or equal to 65 years, 30% aged 45-64 years, and 10% aged 20-44 years. The mean age-adjusted annual incidence was 2.4 per 1000 persons with diabetes (range: 2.1-2.6), and the age-adjusted female-to-male rate ratio was 1.4:1. Overall, incidence remained stable during 1987-1994 (Figure_1); however, for both men and women aged 20-44 years, incidence decreased approximately 29%. In 1994, the overall prevalence of blindness caused by diabetes recorded on the MCB register was 3434 cases; the annual mean for 1987-1994 was 2994 (range: 2298-3536). Persons aged greater than or equal to 65 years accounted for 67% of cases, persons aged 45-64 years for 23%, and persons aged 20-44 years for 10%. The mean age-adjusted annual prevalence was 18.5 per 1000 persons with diabetes (range: 15.3-20.2), and the age-adjusted female-to-male rate ratio was 1.4:1. During 1987-1994, the overall age-adjusted prevalence increased 28% (Figure_2). Prevalence decreased 17% among persons aged 20-44 years and increased substantially (46%) among persons aged greater than or equal to 65 years. Reported by: M El-Hashimy, MD, K Alich, MS, Diabetes Control Program, Massachusetts Dept of Public Health. Epidemiology and Statistics Br, Div of Diabetes Translation, National Center for Chronic Disease Prevention and Health Promotion, CDC. Editorial NoteEditorial Note: A substantial proportion of the visual loss caused by diabetes is preventable. Early detection of diabetic retinopathy and timely intervention with laser photocoagulation can reduce the incidence of severe vision loss by 50%-60% in patients with macular edema and by 90% in patients with proliferative retinopathy (4). In Massachusetts, the reported decline in the incidence of blindness among persons with diabetes aged 20-44 years may reflect early detection of and treatment for diabetic retinopathy or improved glycemic control. However, young persons with diabetes account for only a small proportion of total cases of blindness among the adult population with diabetes. In Massachusetts, the overall stable incidence and increasing prevalence of blindness caused by diabetes may have reflected low rates for persons with diabetes who received the recommended annual eye screening examination for diabetic retinopathy (5) and underscore the need for intensification of screening for diabetic retinopathy in persons with diabetes. The increase in prevalence during 1987-1994 also may reflect improved case ascertainment and reporting or increased survival among persons with diabetes. For example, in Massachusetts from 1987 to 1994, the estimated mean survival of blind persons with diabetes from time of diagnosis of blindness to death increased from 6.8 years to 8.7 years, consistent with previous estimates of survival among persons with diabetes who are legally blind (6). A major limitation of using data from the MCB registry is that completeness of reporting to the registry has not been determined. Despite the availability of incentives for persons who are registered (e.g., tax deductions and exemptions), some degree of underreporting is expected and is a well-recognized limitation of blindness registries (7,8). Reasons for underreporting include a lack of awareness among both patients and health-care providers of the need for or benefits of reporting, concern about lack of confidentiality of medical information, and social stigma associated with blindness. However, levels of reporting of cases of blindness caused by diabetes may be high: during 1993-1994, at least 90% of ophthalmologists in Massachusetts reported cases to MCB (M. El-Hashimy, Massachusetts Department of Public Health, personal communication, 1995). Furthermore, except for persons aged greater than or equal to 65 years, the incidence rates of blindness in the MCB registry were comparable to those for persons in the Wisconsin Epidemiologic Study of Diabetic Retinopathy for 1980-1992 (aged 20-24 years, 1.9 and 1.9, respectively; aged 45-64 years, 1.8 and 2.3, respectively; aged greater than or equal to 65 years, 2.9 and 5.7, respectively; and overall, 2.4 and 3.9, respectively) *** (S. Moss, R. Klein, University of Wisconsin Medical School, personal communication, 1996). This comparability of incidence rates for persons with diabetes aged less than 65 years suggests that completeness of reporting to MCB is high and supports the use of MCB findings for developing national estimates of the incidence of blindness caused by diabetes. MCB, the Diabetes Control Program of the Massachusetts Department of Public Health, and CDC are collaborating to improve the level and quality of reporting of blindness in Massachusetts. Based on findings of a survey to identify factors associated with nonreporting by eye-care providers in Massachusetts (9), a comprehensive strategy has been initiated to increase awareness of the importance and benefits of reporting. This strategy has included the development and distribution of educational materials for eye-care providers, patients, and patients' families. In addition, providers must report the diabetes status of all new registrants, and coding practices have been changed to more accurately reflect specific causes of blindness caused by diabetes. References
* For blindness among persons with diabetes, site/type codes 952-954, 957, 962-964, 967, and 620, and etiology codes 6210, 9501, and 9503. ** Age-specific diabetes prevalence estimates for whites were used to generate conservative estimates of the number of persons with diabetes because age-specific intercensal population estimates were not available for separate race groups. *** Per 1000 persons with diabetes. Age-adjusted to the estimated number of persons with diabetes in Massachusetts in 1987. Figure_1 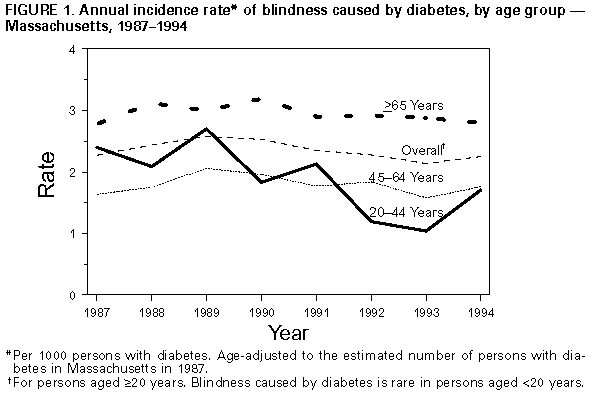 Return to top. Figure_2 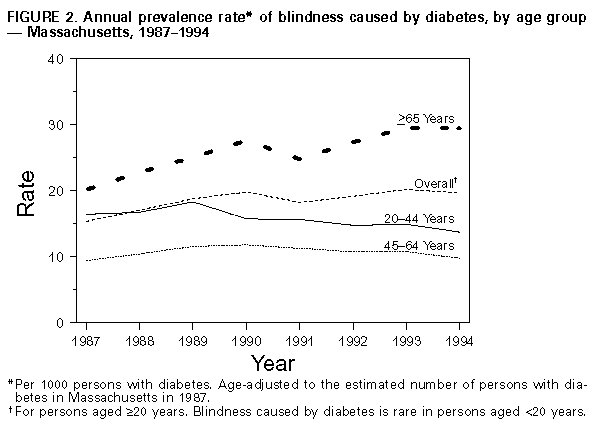 Return to top. Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 09/19/98 |
|||||||||
This page last reviewed 5/2/01
|
{kind=link}
{kind=link}