 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Average Postpartum Length of Stay for Uncomplicated Deliveries -- New Jersey, 1995During 1970-1992, total lengths of hospital stay following delivery declined substantially for both mothers and newborn infants (1). In response to public perceptions that postpartum stays have become excessively short, 28 states have enacted legislation and the U.S. Senate is considering legislation * mandating that insurers provide health-care coverage for a minimum postpartum length of stay for both mother and infant. On June 28, 1995, New Jersey enacted legislation requiring insurance companies and health-maintenance organizations (HMOs) to pay for at least a 48-hour postpartum hospital stay for women and newborns following vaginal delivery and a 96-hour postpartum stay following cesarean delivery when requested by the mother or the attending physician. ** To assess the effect of this law in New Jersey on the average length of stay for uncomplicated deliveries, electronic birth certificate (EBC) data for 1995 were analyzed from four New Jersey hospitals. This report summarizes the findings, which demonstrate that, following enactment of legislation, the average length of stay increased for uncomplicated deliveries at these four hospitals. On January 17, 1995, New Jersey initiated pilot testing of an EBC system in four of the state's 73 facilities that perform deliveries (69 hospitals and four birthing centers). These four hospitals, representing approximately 8% of births in New Jersey, were selected because they were considered sufficiently diverse to test the system and to detect any problems before statewide implementation of the EBC system in all birthing facilities (V. Dato, Division of Family Health Services, New Jersey Department of Health and Senior Services, personal communication, September 1995). The selected hospitals (one regional perinatal center and three community hospitals) are nonprofit organizations and represent north, south, and central New Jersey and urban and suburban areas. Because the EBC data include the exact time of delivery and the day and hour of discharge for the infant, length of stay was calculated in hours and converted to the equivalent proportion of days. Length of stay was defined as the time from birth to discharge of an infant from the hospital. Deliveries were classified as uncomplicated if they met the following criteria: 1) a live-born infant weighing greater than or equal to 2500 g (greater than or equal to 5 lbs 8 oz) was delivered vaginally or by cesarean, 2) the mother and infant were discharged on the same day, and 3) the infant was not admitted or transferred to a neonatal intensive-care unit. Because this study focused on length of stay for uncomplicated deliveries, deliveries with a high likelihood of having complications (i.e., those greater than the 97.5th percentile for length of stay) were excluded from analysis. *** From January 17 through December 31, 1995, a total of 9007 live-born infants were delivered at the four selected hospitals in New Jersey. Of the 7209 uncomplicated deliveries, 5619 (78%) were vaginal, and 1590 (22%) were cesarean. The number of deliveries that occurred before and after the law were similar: for vaginal deliveries, 46% and 54% of deliveries, respectively, and for cesarean deliveries, 47% and 53%, respectively. After enactment of the New Jersey legislation, the average postpartum length of stay increased for both uncomplicated vaginal and cesarean deliveries (Figure_1). The average length of stay for vaginal deliveries increased 29%, from 1.4 days before the law to 1.8 days after the law (Table_1). The average length of stay for cesarean deliveries increased 18%, from 2.8 days before the law to 3.3 days after the law. Length of stay also was examined by type of insurance and hospital (Table_1). After enactment of the law, length of stay increased for all types of insurance; increases were greater for private and federal assistance insurance **** than for self-pay groups. However, self-pay deliveries represented less than 2% of all deliveries. Length of stay also increased for all four participating hospitals after enactment of the law; the increase was greatest for the hospital with the shortest average length of stay for cesarean deliveries before enactment of the law. Reported by: V Dato, MD, L Ziskin, MD, M Fulcomer, PhD, RM Martin, MPH, K Knoblauch, New Jersey Dept of Health and Senior Svcs. Pregnancy and Infant Health Br, Div of Reproductive Health, National Center for Chronic Disease Prevention and Health Promotion, CDC. Editorial NoteEditorial Note: The findings in this report indicate that, after enactment of legislation in New Jersey mandating insurance coverage for a minimum length of hospital stay for mother and infant following obstetric delivery, the average postpartum length of stay for all uncomplicated deliveries increased by 10-12 hours in these four hospitals. Because the New Jersey EBC system allowed calculation of the length of stay in hours, the system provides a more precise measure of the length of stay than most previous studies, which calculated length of stay in days. The findings in this report are subject to at least three limitations. First, EBC data are subject to the limitations of other vital records data, including limited information (particularly about content of prenatal care). Second, because the analysis included only the four hospitals using the EBC system for the 6 months before enactment of the New Jersey legislation, the results may not be generalizable to the entire state. Finally, some insurance carriers administer both traditional health-care plans, which are subject to state regulation, and self-insured health plans, which are not. Therefore, for deliveries covered by these carriers, the EBC system cannot differentiate those deliveries exempt from the state law. Following consumer demand for less medical intervention in the birthing process (2) and institution of cost-containment measures by the insurance industry, the national average length of hospital stay for obstetric deliveries declined by nearly 50% during 1970-1992. In 1992, the average total length of stay for all hospital deliveries in the United States was 2.6 days (2.1 days for vaginal deliveries and 4.0 days for cesarean deliveries) (1). In the western United States, lengths of stay of 12-24 hours after uncomplicated vaginal deliveries are common (3). However, consumer groups, legislators, and health-care providers are concerned that early hospital discharge may adversely affect 1) the mother's feeling of preparedness to care for the infant and herself, 2) the ability of hospital staff to effectively teach a mother to care for the infant and herself and assess her ability to do so, 3) initiation and continuation of breastfeeding, 4) early diagnosis and treatment of infant and maternal morbidity, and 5) the ability to obtain adequate specimens for newborn metabolic screenings (3). Over the past several decades, early postpartum discharge has been variously defined (4). In 1992, the American Academy of Pediatrics (AAP) and the American College of Obstetricians and Gynecologists defined early discharge for uncomplicated deliveries as less than 48 hours for vaginal delivery and less than 96 hours for cesarean delivery (5). In addition, in 1995, the AAP published guidelines for newborn discharge (6) that include meeting certain medical criteria and receiving appropriate support and follow-up. However, previous studies have not adequately examined the effects of short postpartum stays on maternal and infant outcomes because of small sample sizes, poor study designs, and lack of controls. In addition, most of these studies were conducted under specific, controlled circumstances (e.g., intensive and repeated in-home follow-ups) that do not represent well-established standards of care for health-care providers (3). Further research is needed to determine an optimal length of stay and adequate follow-up care for women and infants. Because of federal legislation enacted in 1974 (Employee Retirement Income Security Act of 1974 {ERISA} ***** ), state legislation cannot mandate coverage requirements for employer self-insured plans. An estimated 40%-55% of the insured U.S. population is covered by ERISA plans (7). The proposed New Borns' and Mothers' Health Protection Act of 1996 would require a minimum coverage for postpartum stays of 48 hours for vaginal deliveries and 96 hours for cesarean deliveries for all insurance plans in all states. References
* The New Borns' and Mothers' Health Protection Act of 1996; S. Rep. No. 969, 104th Cong., 2d Sess. (1996). ** N.J. Stat. Ann. 17:48-61 as amended by Public Law 1995, c. 138. *** Deliveries for which the length of stay was greater than the 97.5th percentile for the four hospitals were identified using distributions specific for type of delivery and occurrence before or after enactment of the law. For vaginal deliveries, postpartum lengths of stay that were greater than 2.5 days before the law and greater than 2.8 days after the law were excluded from analysis and, for cesarean deliveries, postpartum lengths of stay greater than 4.4 days before the law and greater than 5.1 days after the law were excluded. The resulting distributions of length of stay for uncomplicated deliveries were approximately normal. **** Includes Medicaid, Medicare, and other federal programs. ***** Public Law 93-406 (29 USC 1001-1461). Figure_1 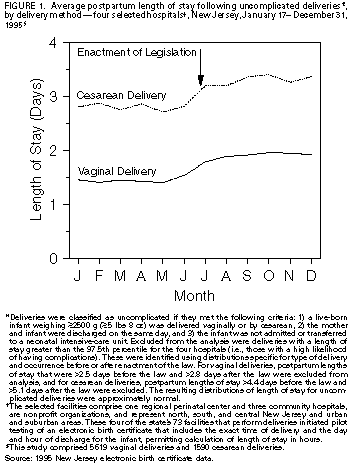 Return to top. Table_1 Note: To print large tables and graphs users may have to change their printer settings to landscape and use a small font size.
TABLE 1. Average postpartum length of stay * (LOS) following uncomplicated deliveries + before and after enactment of New
Jersey legislation, by delivery method and selected characteristics -- four selected hospitals, & New Jersey,
January 17-December 31, 1995
===============================================================================================================================================
Vaginal Cesarean
-------------------------------------------- -----------------------------------------------
Average LOS Average LOS
---------------------- Absolute ---------------------- Absolute
Before law After law change Percentage Before law After law change Percentage
Characteristic (n=2582) (n=3037) (days) change (n=754) (n=836) (days) Change
---------------------------------------------------------------------------------------------------------------------
Mother's insurance @
Private ** 1.4 1.8 0.4 29 2.8 3.3 0.5 18
Federal assistance ++ 1.3 1.8 0.5 38 2.7 3.3 0.6 22
Self-pay 1.3 1.7 0.4 31 2.8 3.0 0.2 7
Hospital
1 1.3 1.8 0.5 38 2.9 3.3 0.4 14
2 1.3 1.9 0.6 46 2.3 3.1 0.8 35
3 1.3 1.7 0.4 31 3.1 3.2 0.1 3
4 1.5 1.9 0.4 27 3.0 3.5 0.5 17
Total 1.4 1.8 0.4 29 2.8 3.3 0.5 18
---------------------------------------------------------------------------------------------------------------------
* In days.
+ Deliveries were classified as uncomplicated if they met the following criteria: 1) a live-born infant weighing >=2500 g (>=5 lbs 8 oz) was
delivered vaginally or by cesarean, 2) the mother and infant were discharged on the same day, and 3) the infant was not admitted
or transferred to a neonatal intensive-care unit. Excluded from the analysis were deliveries with a length of stay greater than the
97.5th p�ercentile for the four hospitals (i.e., those with a high liklihood of having complications. These were identified using
distributions specific for type of delivery and occurrence before or after enactment of the law. For vaginal deliveries, postpartum
lengths of stay that were >2.5 days before the law and >2.8 days after the law were excluded from analysis, and for cesarean deliveries,
postpartum lengths of stay >4.4 days before the law and >5.1 days after the law were excluded. The resulting distribution of length
of stay for uncomplicated deliveries were approximately normal.
& The selected facilities comprise one regional perinatal center and three community hospitals, are nonprofit organizations, and
represent north, south, and central New Jersey and urban and suburban areas. These four of the state's 73 facilities that perform
deliveries initiated pilot testing of an electronic birth certificate that includes the exact time of delivery and the day and hour of
discharge for the infant, permitting calculation of length of stay in hours.
@ Data were excluded for 1256 mothers (971 who had vaginal deliveries and 285 who had cesarean deliveries) whose insurance was
categorized as "Other/Unknown insurance," and for 311 mothers (238 who had vaginal deliveries and 73 who had cesarean deliveries)
for whom insurance information was missing.
** Includes commercial insurers, preferred-provider organizations, health-maintenance organizations (HMOs), and Medicaid HMOs.
++ Medicaid, Medicare, and other federal programs.
===============================================================================================================================================
Return to top. Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 09/19/98 |
|||||||||
This page last reviewed 5/2/01
|
{kind=link}