 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Shigella sonnei Outbreak Associated with Contaminated Drinking Water -- Island Park, Idaho, August 1995On August 20, 1995, the District 7 Health Department requested the Idaho Department of Health to assist in investigating reports of diarrheal illness among visitors to a resort in Island Park in eastern Idaho; Shigella sonnei had been isolated from stool cultures of some cases. This report summarizes the findings of the investigation, which implicated contaminated drinking water as the cause of the outbreak. The resort is located in an area frequented by tourists because of its recreational waters and proximity to a large national park. Facilities include a 36-room motel, conference room, two hot tubs, and 10 hook-ups for recreational vehicles. The resort does not have a restaurant but offers catered meals to groups. To determine the source and extent of the outbreak, persons who had either stayed overnight or eaten at the resort during August 1-21 were telephoned and interviewed; resort staff also were interviewed. Names of visitors were obtained from the resort's records and from interviews with other guests. A probable case was defined as onset of diarrhea (two or more loose stools during a 24-hour period) with either fever or bloody stools while at the resort or within 11 days of leaving the resort. A confirmed case additionally required Shigella sonnei isolated from stool. Approximately 810 persons stayed or ate at the resort during August 1-21; of these, 222 were contacted, and 221 (99%) agreed to be interviewed. A total of 82 cases (attack rate: 35%) were identified, including 67 probable and 15 confirmed. The median age of case-patients was 31 years (range: 3 months-81 years), and 42 (51%) were male. Onset of illness occurred during August 6-24 (Figure_1). The average duration from time of arrival until onset of diarrhea was 4 days (range: 1-11 days). Fifteen patients (18%) had bloody diarrhea, eight sought treatment in local emergency departments, and five were admitted to local hospitals. Risk for illness was higher among persons who had drunk tap water or had used ice from the ice machines at the resort than among those who did not (80 {46%} of 175 versus one {3%} of 39; relative risk=17.6; 95% confidence interval=2.5-123.0). Increased risk for illness was not associated with eating or drinking any resort food or beverages (other than water), swimming or fishing in the area recreational waters, using a hot tub, or dining in any local restaurants in Island Park. At least 14 of the case-patients stayed only one night at the resort and had drunk tap water obtained in their rooms but had not eaten food prepared at the resort. After receiving reports of diarrheal illness among guests at the resort, the District 7 Health Department recommended several prevention measures before initiating the investigation. On August 17, the resort posted warning signs at water taps cautioning against drinking water; on August 19, food service was terminated; and on August 21, bottled water was placed in every room. Resort water is supplied by one well, which was dug in 1993. Samples of water obtained from the well on August 23 were positive for fecal coliform bacteria; however, cultures were negative for Shigella. During the outbreak investigation, residents in some houses in a new subdivision adjacent to the resort reported acute diarrheal illness. Each house either had a private well or shared a well with a neighbor. S. sonnei was isolated from stool samples from six persons who resided in three of these homes. All six persons denied direct contact with other neighbors or visiting the resort. Fecal coliform bacteria were identified in samples obtained from six of 10 neighborhood wells during August 21-23. However, cultures of water samples from two of these wells were negative for S. sonnei. The water table in the area was substantially higher than normal because of high rainfall levels during the spring. Initial inspection of a sewer line that had been placed from the subdivision and the resort by a private developer indicated that sewage was draining improperly, although no breaks were identified in selected sections that were excavated for inspection. Plasmid profiles were performed on Shigella isolates from 15 ill resort visitors, two ill staff members, and five of six ill residents of the neighboring houses; all 22 isolates shared seven identical plasmids. S. sonnei isolates obtained from patients elsewhere in Idaho did not match this pattern. The District 7 Health Department required that the resort provide bottled or boiled water to visitors and recommended that persons residing in the area have their well water tested and boil all drinking water. Since the investigation, the resort has drilled a new and deeper well. Reported by: B Arnell, District 7; J Bennett, Southeast District; R Chehey, State Bur of Laboratories; J Greenblatt, MD, State Epidemiologist; Idaho State Dept of Health. Foodborne and Diarrheal Diseases Br, Div of Bacterial and Mycotic Diseases, National Center for Infectious Diseases; Div of Field Epidemiology, Epidemiology Program Office, CDC. Editorial NoteEditorial Note: S. sonnei is a well-recognized cause of gastrointestinal illness and the most common cause of bacillary dysentery in the United States. In addition to diarrhea, common manifestations of shigellosis include fever, abdominal pain, and blood or mucus in the stool. Although most outbreaks of shigellosis have been attributed to person-to-person transmission (1), foodborne (2-4), waterborne (5), and swimming-related (6,7) outbreaks have been reported. Waterborne outbreaks commonly are associated with wells that have been fecally contaminated. However, because Shigella organisms rarely are isolated from water sources, the identification of a waterborne source usually is based on epidemiologic evidence. The findings of this investigation indicate possible transmission from multiple wells in the same area, suggesting possible contamination and spread of viable Shigella organisms through the groundwater. Plasmid profile analysis confirmed that the outbreak isolates were the same strain that caused illness among persons in the neighboring community. Although investigation of the sewer line continues, the source of the contamination of the well water has not yet been determined. Routine water-quality testing, including testing for fecal coliform (thermotolerant) bacteria, is the most practical indicator of possible bacterial contamination of drinking water from both community and private water supplies. However, many privately owned wells never are tested for fecal coliform bacteria. In addition, timely testing, reporting, and follow-up in cases of contaminated public water systems often are constrained because of limited resources available to local health departments. References
Figure_1 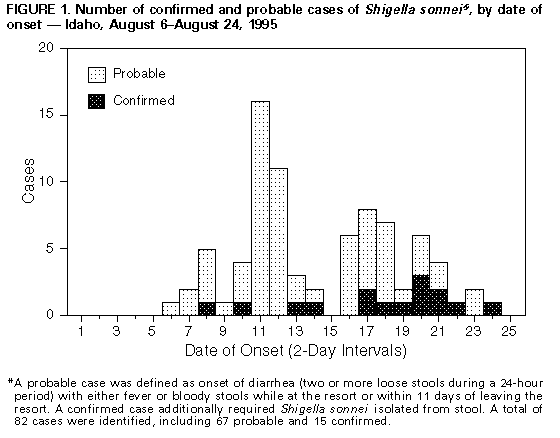 Return to top. Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 09/19/98 |
|||||||||
This page last reviewed 5/2/01
|
{kind=link}