 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Progress Toward Global Eradication of Poliomyelitis, 1988-1993In May 1988, the World Health Organization (WHO) adopted a resolution to eradicate poliomyelitis by the year 2000. Since then, all six WHO regions have made substantial progress toward this goal using three major control strategies: 1) maintaining high coverage of children with at least three doses of oral poliovirus vaccine (OPV3); 2) administering supplementary doses of OPV to all young children (generally those aged less than 5 years) during National Immunization Days (NIDs) * and during door-to-door vaccination campaigns in areas where wild poliovirus circulation persists at low levels; and 3) developing sensitive systems of epidemiologic and laboratory surveillance (1). This report summarizes progress of the global polio eradication initiative from 1988 through 1993. ** Worldwide. Reported global vaccination coverage with OPV3 by age 1 year increased from 67% in 1988 to 85% in 1990 but decreased to 80% in 1992 and 81% in 1993 (Figure_1). From 1988 through 1993, reported cases of polio decreased 70%, from 32,286 to 9714 (Figure_1). During these years, there were substantial decreases in the number of countries reporting polio cases (88 {45%} of 196 and 56 {27%} of 209, respectively) and the number of countries reporting 100 or more cases per year (20 {10%} and 11 {5%}, respectively) (Figure_2). In addition, the number of countries reporting zero polio cases increased from 107 (55%) to 144 (69%). *** African Region. Reported coverage with OPV3 increased from 44% in 1988 to 57% in 1991 but decreased to 49% in 1992 and 50% in 1993. From 1988 through 1993, reported cases of polio decreased from 4546 to 1437. The number of countries reporting polio cases remained unchanged (37 {79%} of 47). In 1993, the African region reported 15% of the global total of polio cases. Despite reporting zero polio cases for more than 3 years, Namibia reported an outbreak of 53 cases in 1993, probably as a result of recent importation of wild poliovirus from a polio-endemic area. Region of the Americas. Reported coverage with OPV3 increased from 82% to 86%, while reported cases of polio decreased from 340 to zero; the number of countries reporting polio cases decreased from 13 (28%) to zero of 47. The last confirmed case of paralytic polio caused by wild poliovirus occurred in August 1991 in Peru. Eastern Mediterranean Region. Reported coverage with OPV3 increased from 69% to 75%, while reported cases of polio increased from 2332 to 2451; the number of countries in the region reporting polio decreased from 17 (71%) of 24 to 10 (43%) of 23. In 1993, the Eastern Mediterranean Region reported 25% of the global total of polio cases; 84% of the regional total was reported from Pakistan (74%) and Sudan (10%). In 1993, Pakistan and Sudan experienced large outbreaks (1803 and 252 reported cases, respectively), primarily among unvaccinated children. Despite OPV3 coverage of more than 85% and no reported cases for at least 2 years, small outbreaks of type 1 also occurred in Oman during 1988 and 1993 and in Jordan during 1991-92; all three outbreaks were caused by importation of wild poliovirus from other polio-endemic countries. European Region. Reported coverage with OPV3 decreased from 86% to 72%, while reported cases of polio decreased from 206 to 198; the number of countries reporting polio cases increased from seven (23%) of 31 to 12 (24%) of 50. In 1993, the European Region reported 2% of the global total of polio cases; 83% of the regional total was from republics of the former Soviet Union. Azerbaijan and Uzbekistan experienced outbreaks in 1993 (70 and 68 reported cases, respectively), primarily among unvaccinated children. Despite coverage of 97% with three doses of inactivated poliovirus vaccine and no reported polio cases for more than 10 years, the Netherlands experienced an outbreak of 71 cases during 1992-93 among members of a religious group who do not routinely accept vaccination, caused by importation of wild poliovirus that originated from the Indian subcontinent. Southeast Asia Region. Reported coverage with OPV3 increased from 57% to 90%, while reported cases of polio decreased from 22,814 to 4414. The number of countries in the region reporting polio cases decreased from nine (82%) to seven (64%) of 11. In 1993, the Southeast Asian Region reported 45% of the global total of polio cases; 93% of the regional total was from India. Western Pacific Region. Reported coverage with OPV3 increased from 89% to 93%, while reported cases of polio decreased from 2079 to 1214; the number of countries reporting polio cases decreased from six (17%) to five (14%) of 35. In 1993, the Western Pacific Region reported 13% of the global total of polio cases; 88% of the regional total was from the People's Republic of China (54%) and Vietnam (34%). Despite OPV3 coverage of 90% and no reported polio cases for 5 years, Malaysia experienced a small outbreak in 1992 caused by importation of wild poliovirus that originated from the Indian subcontinent. Reported by: Expanded Program on Immunization, Global Program for Vaccines, World Health Organization. Polio Eradication Activity, National Immunization Program; Div of Viral and Rickettsial Diseases, National Center for Infectious Diseases; International Health Program Office, CDC. Editorial NoteEditorial Note: Since 1988, the global incidence of paralytic polio has decreased substantially, and polio apparently has been completely eliminated from the Region of the Americas (1,2). The number of polio cases reported in 1993 represents a 33% decrease compared with 1992 and a 70% decrease compared with 1988. Furthermore, nearly three quarters of all countries reported zero cases of polio in 1993, and polio-free zones are present or emerging in the Americas, northern, southern, and eastern Africa, the Arabian peninsula, western and central Europe, and the Western Pacific (Figure_2). Despite this substantial progress overall, paralytic polio remains highly endemic throughout the Indian subcontinent and continues to occur in most countries of sub-Saharan Africa and Asia, including many republics of the former Soviet Union (Figure_2). In 1993, nearly two thirds of all polio cases reported worldwide were from the Indian subcontinent, including 42% from India, 19% from Pakistan, and 2% from Bangladesh. Lower than optimal levels of routine vaccination coverage, pockets of unvaccinated children within otherwise highly vaccinated populations, crowding, poor sanitation, and suboptimal seroconversion to poliovirus types 1 and 3 following three routine doses of OPV in many tropical and subtropical regions probably contribute to ongoing wild poliovirus transmission in these areas (1,3). In addition to remaining areas of endemic transmission, outbreaks of paralytic polio have recently occurred in several countries 2 or more years after the last reported case of polio, despite high levels of routine vaccination coverage (4,5). Genotypic comparisons between wild poliovirus strains in the global laboratory network have demonstrated that outbreaks in Oman (1988- 89 and 1993), Jordan (1991-92), Malaysia (1992), and the Netherlands (1992-93) occurred as a result of importation of wild poliovirus from polio-endemic countries in the Indian subcontinent (4,5). Thus, until polio is eradicated globally, every polio-free country may be at risk for importation of wild poliovirus from remaining polio-endemic reservoirs. Routine vaccination alone is probably insufficient to eliminate wild poliovirus transmission in most countries, and supplementary vaccination activities, including NIDs, are necessary in countries where polio remains endemic (1,2,6-10). In 1993 and early 1994, NIDs were conducted for the first time in China, Vietnam, Philippines, Laos, Iran, and Pakistan, which together accounted for 31% of all polio cases reported globally; by the end of 1994, at least 63 (30%) of 209 countries will be conducting NIDs as a polio-control strategy. As more countries adopt this strategy, further progress is expected toward global eradication of polio. Despite substantial progress toward global eradication of polio, several challenges remain, including 1) reversing the decline in global routine vaccination levels; 2) increasing vaccination levels in unvaccinated subpopulations; 3) preventing the reintroduction of wild poliovirus into polio-free areas by eliminating reservoirs in polio-endemic countries (particularly the Indian subcontinent); 4) increasing the awareness of donor agencies and governments in industrialized countries of the substantial financial and humanitarian benefits of global eradication of polio, thus engendering support from unaffected countries beyond that already provided by organizations such as Rotary International; 5) encouraging all countries that remain polio-endemic to make polio eradication a priority activity, including the implementation of NIDs and the initiation of acute flaccid paralysis surveillance; and 6) providing support to vaccination program managers for training to develop managerial skills for implementing and maintaining effective vaccination and surveillance programs in all countries. The success of the polio eradication initiative will depend on finding solutions to these financial, managerial, political, and technical challenges. References
* Mass campaigns over a short period (days to weeks) in which two doses of OPV are administered to all children in the target age group, regardless of prior vaccination history, with an interval of 4-6 weeks between doses. ** Based on surveillance data submitted to WHO as of July 1, 1994. *** The difference between the number of countries reporting polio cases or zero cases and the total number of countries reflects those not submitting reports. Figure_1 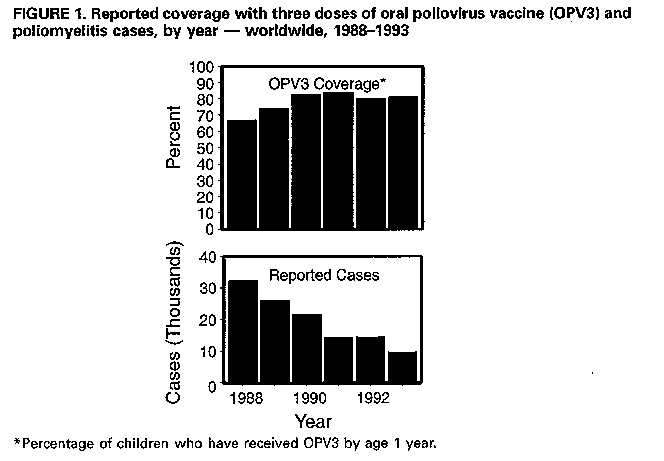 Return to top. Figure_2 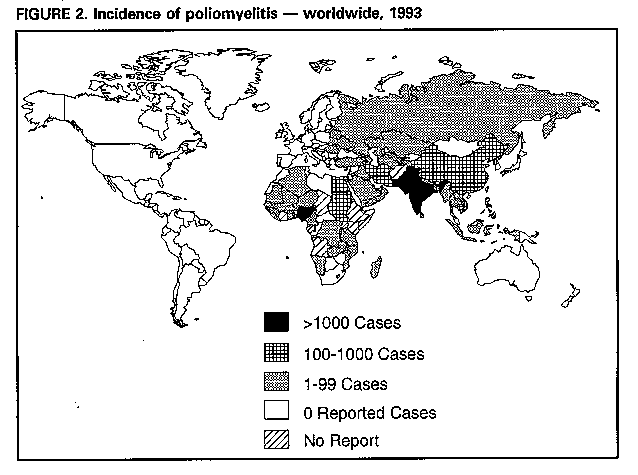 Return to top. Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 09/19/98 |
|||||||||
This page last reviewed 5/2/01
|
{kind=link}
{kind=link}