 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
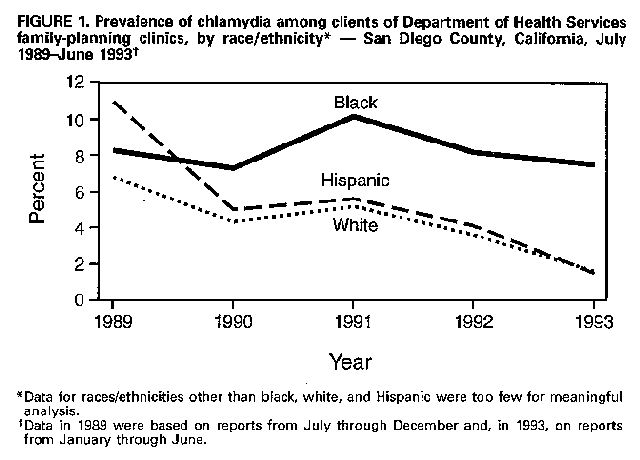
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Epidemiologic Notes and Reports Chlamydia Prevalence and Screening Practices -- San Diego County, California, 1993Chlamydia trachomatis is the most common bacterial sexually transmitted disease in the United States and causes an estimated 4 million infections annually (1). Approximately 70% of infected women have few or no symptoms (2), and asymptomatic infection in women can persist for up to 15 months (3). Infection can progress to involve the upper reproductive tract and may result in serious complications. To identify women who may have chlamydial infections, CDC has recommended routine testing based on age, risk behavior, and clinical findings -- especially in clinics and group practices that provide reproductive health care to adolescent and young women (4). This report describes the prevalence of chlamydial infections among patients visiting the family-planning clinic service of the San Diego County Department of Health Services from July 1989 through June 1993 and summarizes the findings of a survey in May 1993 that assessed chlamydia screening, reporting, and treatment practices for women who attended primary-care community-based clinics and group practices in San Diego County. Prevalence of Chlamydial Infections The San Diego County Department of Health Services provides family-planning services in San Diego County in six public health centers. Each clinic follows a written protocol that requires screening of all clients during their initial visit and recommends screening for clients during annual visits -- particularly for those whose sexual behavior increases their risk for infection. From March 1989 through February 1991, endocervical specimens were tested at the San Diego County Public Health Laboratory using the Chlamydia Antigen ELISA (Ortho Diagnostic Systems, Inc. *, Raritan, New Jersey); beginning March 1991, specimens were tested using the MicroTrak EIA (Syva, San Jose, California). The proportion of women screened was determined using data from annual family-planning clinic-service utilization reports. Test results and demographic and limited clinical information were obtained from the laboratory's chlamydia-test database. During July 1989-June 1993, approximately 95% of family-planning clients were tested for Chlamydia during their initial visit, and 70% were tested during their annual visit. Of 11,044 specimens tested, 91% were obtained during routine testing of clients without symptoms. The prevalence of chlamydial infections decreased from 10.0% during July-December 1989 to 1.9% during January-June 1993, a decline of 81.0%. During July 1989-June 1993, the prevalence of chlamydia among black women was 8.5%, more than 1.5 times that among Hispanic (5.3%) and white (4.5%) women. During the 4-year period, the prevalence declined minimally among black women and steadily among white and Hispanic women (Figure_1). Prevalence was inversely related to age, with the highest prevalence among women aged less than 20 years (8.4%); among women aged less than 20 years, the prevalence decreased from 9.9% during July 1989-December 1990 to 4.8% during January 1992-June 1993, a 51.5% decline. Chlamydia-Screening Practices Survey The survey of chlamydia screening and related practices was mailed in May 1993 to all 171 primary-care clinics and group practices in San Diego County that provided women's health services. The survey requested information about chlamydia screening, reporting, diagnosis and treatment practices, types of clinical services, and other chlamydia-related issues. Chlamydia-screening practices were classified as clinician-directed screening (i.e., when testing was based on the clinician's assessment of signs, symptoms, or risk behavior) or as protocol screening (i.e., when clinics followed a policy to test all women of reproductive age or all those aged less than 20 years at their initial or annual visit). Surveys were returned by 85 (50%) of the providers. All providers reported conducting clinician-directed screening; 45 (53%) followed protocol screening in at least one clinical service. Public providers were more likely than private providers to follow protocol screening (60% versus 37%). Protocol screening was used commonly in prenatal services (79%), compared with initial visits for adolescent services (39%), initial visits for family-planning services (33%), and gynecologic services (20%) (Table_1). Among providers following protocol screening, written screening policies had been established most commonly in prenatal services (75%), followed by family-planning (58%) and gynecologic (46%) services. Almost all (greater than or equal to 92%) providers reported testing and immediately treating (i.e., on the same day as their visit and before test results were known) clients who had chlamydia-related syndromes (e.g., pelvic inflammatory disease {PID} or mucopurulent cervicitis) or who had reported a sexual exposure to a Chlamydia-infected person. In California, both PID and chlamydial infections are notifiable conditions; however, only 34 (54%) of the 63 providers who responded to this question routinely reported PID cases, and 55 (75%) of 73 responding providers reported positive chlamydia test results. Reporting practices were similar for private and public providers. DNA probe testing was the most frequently used chlamydia test (47 {58%} of 81). Almost all (74 {97%} of 76) providers who responded reported referring male sex partners for examination and treatment. The most common approaches were on-site examination with presumptive treatment (57%) and health department referral (35%). However, only 14 (18%) of 80 providers reported having a method of following up sex partners' treatment for chlamydia. Reported by: M Mendes, MPH, C Spitters, MD, S Waterman, MD, C Peter, PhD, R Ross, MD, San Diego County Dept of Health Svcs, San Diego; J Felten, MPA, Sexually Transmitted Diseases Br, GW Rutherford, III, MD, State Epidemiologist, California Dept of Health Svcs. Surveillance and Information Systems Br, Div of Sexually Transmitted Diseases and HIV Prevention, National Center for Prevention Svcs; Div of Field Epidemiology, Epidemiology Program Office, CDC. Editorial NoteEditorial Note: The decline in the prevalence of chlamydial infections among women receiving family-planning clinic services in San Diego County during 1989-1993 was consistent with patterns in other areas. For example, findings from a screening demonstration project in Public Health Service Region X (Alaska, Idaho, Oregon, and Washington) indicated that, among the approximately 70,000 women screened annually in public and private family-planning clinics, the prevalence declined from 9.3% in 1988 to 4.2% in 1993 (5). The prevalence also decreased among women attending family-planning clinics in Wisconsin, where a statewide selective screening program has been operated since 1986 (6). Although the low response rate in San Diego County precludes generalization, the results of the screening practices survey suggest that the use of protocol screening was limited. A policy implemented in California in August 1993 by the California Office of Family Planning now requires chlamydia screening for all women undergoing initial examinations and for women at increased risk undergoing annual and limited examinations who seek services at clinics funded by the California Office of Family Planning. To assist health-care providers in developing protocols and policies, CDC has recommended chlamydia screening for 1) all women with mucopurulent cervicitis; 2) all sexually active women aged less than 20 years; and 3) women aged 20-24 years who meet either of two criteria or women aged greater than 24 years who meet both criteria -- a) inconsistent use of barrier contraception or b) a new sex partner or more than one sex partner during the previous 3 months (4). The Preventive Health Amendments of 1992 authorized CDC to develop a national program to prevent infertility resulting from treatable sexually transmitted diseases in women. Findings from San Diego County, Region X, and Wisconsin also suggest that efforts to prevent chlamydia-associated infertility through the delivery of early detection and treatment services -- particularly for women with asymptomatic infections -- may have been effective in reducing the prevalence of chlamydial infections. A new program to prevent infertility will expand services to approximately 800,000 women in the four Public Health Service regions in which chlamydia-prevention projects have been established (Regions III, VII, VIII, and X) and will evaluate critical issues in operational research. Ongoing analysis of surveillance data and other information characterizing chlamydial infection can assist clinical programs in modifying screening practices to ensure effectiveness. In San Diego County, the prevalence of chlamydial infection was higher among black women than women in other racial/ethnic groups; however, information was not obtained about the social and economic status of patients. Therefore, in San Diego County, race should be considered a risk marker rather than a screening criterion for chlamydial infection. Health-care facilities that provide family-planning, adolescent health, and routine gynecologic services to adolescent and young adult women should consider the use of screening protocols for all clients at risk for chlamydial infections. Important components of chlamydia-control programs include treatment and risk-reduction counseling of sex partners of infected persons. In San Diego County, only 18% of providers reported having a method to ensure treatment of sex partners; this finding underscores the need for facilities that provide health care for women to offer examination and treatment services or arrange for appropriate referral for their clients' male sex partners, and establish procedures for follow-up of the status of referrals. Public health agencies may assist health-care providers in developing such referral and follow-up procedures. References
* Use of trade names and commercial sources is for identification
only and does not imply endorsement by the Public Health Service
or
the U.S. Department of Health and Human Services.
TABLE 1. Chlamydia protocol screening * in clinics and group practices providing
women's health services -- San Diego County, May 1993
===========================================================================================================
Private provider + Public provider & Total
----------------------- ------------------------ ------------------------
Protocol Protocol Protocol
screening screening screening
Total --------- Total --------- Total ---------
Clinical service providers No. (%) providers No. (%) providers No. (%)
---------------------------------------------------------------------------------------------------------
Family planning
Initial visit 28 8 (29) 32 12 ( 38) 60 20 (33)
Annual visit 27 5 (19) 32 8 ( 38) 59 13 (22)
Prenatal initial visit 20 12 (60) 18 18 (100) 38 30 (79)
Gynecologic annual visit 39 5 (13) 32 9 ( 28) 71 14 (20)
Adolescent
Initial visit 23 6 (26) 18 10 ( 56) 41 16 (39)
Annual visit 21 3 (14) 17 7 ( 41) 38 10 (26)
---------------------------------------------------------------------------------------------------------
* Screening of all women of reproductive age or all women aged <20 years at their initial or
annual visit.
+ Comprises private group practices (45), hospital-based clinics (three), and health-maintenance
organizations (one).
& Comprises community health centers (18), student health-services centers (six), Planned
Parenthood clinics (four), health department clinics (three), Indian Health Service clinics (two),
military clinics (two), and prison clinics (one).
===========================================================================================================
Return to top. Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 09/19/98 |
|||||||||
This page last reviewed 5/2/01
|
{kind=link}