Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail.
First Reports Evaluating the Effectiveness of Strategies
for Preventing Violence: Firearms Laws
Findings from the Task Force on Community Preventive Services
Prepared by
Robert A. Hahn, Ph.D.1
Oleg O. Bilukha, M.D., Ph.D.1
Alex Crosby, M.D.2
Mindy Thompson Fullilove, M.D.3
Akiva Liberman, Ph.D.4
Eve K. Moscicki, Sc.D.5
Susan Snyder, Ph.D.1
Farris Tuma, Sc.D.5
Peter Briss, M.D.1
1Division of Prevention Research and Analytic Methods
Epidemiology Program Office
2Division of Violence Prevention
National Center for Injury Prevention and Control, CDC
Atlanta, Georgia
3New York State Psychiatric Institute, Columbia University
New York, New York
4National Institute of Justice
U.S. Department of Justice
Washington, D.C.
5National Institute of Mental Health
National Institutes of Health
Bethesda, Maryland
The material in this report was prepared by the Epidemiology Program Office, Stephen B. Thacker, M.D., Director; Division of Prevention Research and Analytic Methods, Richard E. Dixon, M.D., Director.
Summary
During 2000--2002, the Task Force on Community Preventive Services (the Task Force), an independent nonfederal
task force, conducted a systematic review of scientific evidence regarding the effectiveness of firearms laws in preventing
violence, including violent crimes, suicide, and unintentional injury. The following laws were evaluated: bans on specified firearms or ammunition, restrictions on firearm acquisition, waiting periods for firearm acquisition, firearm registration and licensing
of firearm owners, "shall issue" concealed weapon carry laws, child access prevention laws, zero tolerance laws for firearms
in schools, and combinations of firearms laws. The Task Force found insufficient evidence to determine the effectiveness of any
of the firearms laws or combinations of laws reviewed on violent outcomes. (Note that insufficient evidence to
determine effectiveness should not be interpreted as evidence of ineffectiveness.) This report briefly describes how the reviews
were conducted, summarizes the Task Force findings, and provides information regarding needs for future research.
Background
Although firearms-related* injuries in the United States have declined since 1993, they remained the second leading cause
of injury mortality in 2000, the most recent year for which complete data are available
(1). Of 28,663 firearms-related deaths in 2000 --- an average of 79 per day---16,586 (57.9%) were suicides, 10,801 (37.7%) were homicides, 776 (2.7%) were unintentional, and an additional 500 (1.7%) were legal interventions or of undetermined intent.
An estimated 24.3% of the 1,430,693 violent crimes (murder, aggravated assault, rape, and robbery) committed in
the United States in 1999 were committed with a firearm
(2). In the early 1990s, rates of firearms-related homicide, suicide,
and unintentional death in the United States exceeded those of 25 other high-income nations (i.e., 1992 gross national product
US $8,356 per capita) for which data are available
(3). In 1994, the estimated lifetime medical cost of all firearms injuries in
the United States was $2.3 billion (4).
Approximately 4.5 million new firearms are sold each year in the United States, including 2 million handguns. In
addition, estimates of annual secondhand firearms transactions (i.e., sales, trades, or gifts) range from 2 million to 4.5 million
(5,6). Further, an estimated 0.5 million firearms are stolen annually
(6). Thus, the total number of firearms transactions could be as high as 9.5 million per year.
The 1994 National Survey of the Private Ownership of Firearms (NSPOF), conducted by Chilton Research Services for
the Police Foundation, under sponsorship of the National
Institute of Justice, indicated that American adults
owned approximately 192 million working firearms, an average of one per adult
(7). The NSPOF also indicated that firearm ownership was unevenly distributed in the population: only 24.6% of U.S. adults owned a firearm (41.8% of men and 9.0% of women). Another survey (2) found that 41% of adult respondents reported having a firearm in their home in 1994, and
35% did so in 1998. A third survey (8) reported that 35% of homes with children aged <18 years had at least one firearm. Rates
of firearm ownership in the United States also exceed those of 14 other nations for which data are available, with the exception
of Finland (9).
Of the estimated 192 million firearms owned in the United States at the time of the 1994 NSPOF survey, 65 million
were handguns; 70 million, rifles; 49 million, shotguns; and the remainder were other guns
(7). Among handgun owners, 34.0% kept their guns loaded and unlocked. An estimated 10 million handguns, one sixth of the handguns owned, were
regularly carried by their owners, approximately half in the owners' cars and the other half on the owners'
persons.
The manufacture, distribution, sale, acquisition, storage, transportation, carrying, and use of firearms in the United States
are regulated by a complex array of federal, state, and local laws and regulations.
This review examines firearms laws as one of many approaches to reducing firearms violence
(10,11).
Introduction
The independent, nonfederal Task Force on Community Preventive Services (the Task Force) is developing the
Guide to Community Preventive Services (the
Community Guide) with the support of the U.S. Department of Health and Human
Services (DHHS) in collaboration with public and private partners. Although CDC provides staff support to the Task Force
for development of the Community Guide, the
conclusions presented in this report were developed by the Task Force and are
not necessarily the conclusions of DHHS or CDC.
This report is one in a series of topics included in the
Community Guide, a resource that includes multiple systematic
reviews, each focusing on a preventive health topic. A short overview of the process used by the Task Force to select and review evidence and summarize its findings is included in this report. A full report on the findings and additional evidence
(including discussions of possible additional benefits, potential harms, existing data problems, research gaps, and directions for future research) will be published in the American Journal of Preventive
Medicine.
Methods
The Community Guide's methods for conducting systematic reviews and linking evidence to recommendations have
been described elsewhere (12). In brief, for each
Community Guide topic, a multidisciplinary team (the systematic
review development team) conducts a review consisting of the following steps:
developing an approach to organizing, grouping, and
selecting the interventions to be reviewed;
systematically searching for and retrieving evidence;
assessing the quality of and summarizing the strength of the body of evidence of effectiveness;
assessing cost and cost-effectiveness evidence, identifying applicability and barriers to implementation (if the
effectiveness of the intervention has been established);
summarizing information regarding evidence of other
effects; and
identifying and summarizing research gaps.
Firearms laws were identified as high-priority interventions for violence prevention review in April 1997 by a group
of consultants† representing diverse experience. The group generated a comprehensive list of strategies and created a priority list of interventions for review on the basis of 1) the potential to reduce violence in the U.S. population; 2) the potential benefits
of expanding use of seemingly effective, but underutilized, interventions and reducing use of seemingly ineffective,
but overutilized, interventions; 3) current interest in this intervention among potential audiences; and d) diversity of
intervention types.
The interventions included in this review address several of the objectives outlined in
Healthy People 2010 (13), the
disease prevention and health promotion agenda for the United States. Many of the
Healthy People 2010 objectives outlined in
Chapter 15, "Injury and Violence Prevention," relate to firearms laws and their proposed effects on violence-related outcomes (Box).
To be included in the review of effectiveness, studies had to 1) be a primary evaluation of the selected intervention rather than, for example, a guideline or review; 2) provide
information on at least one outcome of interest from the list of
violent outcomes preselected by the systematic review development team; 3) be conducted in Established Market
Economies§; and 4) compare outcomes in groups of persons exposed to the intervention with outcomes in groups of persons not exposed or less exposed to the intervention (whether the comparison was concurrent between groups or before-and-after within the same group).
Electronic searches for any research published before July 2001 were conducted in MEDLINE, EMBASE,
ERIC, National Technical Information Service (NTIS), PsychINFO, Sociological Abstracts, National Criminal Justice
Reference Service (NCJRS), Public Affairs Information Service (PAIS), Criminal Justice Index, and Gale Group Legal Research
Index.¶ The references listed in all retrieved articles were also reviewed, and specialists on the systematic review development team
and elsewhere were consulted to identify additional reports. Journal articles, government reports, books, and book chapters
were included in this review.
Because the purpose of this review was to assess the effectiveness of firearms laws in preventing violence, studies of firearms
laws were reviewed only if they assessed at least one violent outcome. The outcome measures evaluated to determine the effect of each intervention were violent crimes (i.e., murder, aggravated assault, robbery, and rape), suicide, and unintentional firearm
injury. Aggravated assault was considered a health-related outcome insofar as it is "an unlawful attack by one person upon another for the purpose of inflicting severe or aggravated bodily injury"
(2). Similarly, robbery was considered a health-related outcome insofar
as
it is "the taking or attempting to take anything
of value from the care, custody, or control of a person or persons by force or
threat of force or violence or by putting the victim in fear"
(2). For each of the firearms laws, the team developed an analytic
framework indicating possible causal links between that intervention and one or more of the predefined outcomes of interest.
Each study meeting the inclusion criteria was evaluated with a standardized abstraction form
(14) and was assessed for suitability of study design and threats to validity
(12). On the basis of the number of threats to validity, studies
were characterized as having good, fair, or limited execution. Results for each outcome of interest were obtained from each study that met the minimum quality criteria. Measures that were adjusted for the effects of potential confounders were used in preference to crude effect measures. If two or more studies of a firearms law overlapped in terms of population, time period, and outcomes studied, the systematic review development team chose the study with the fewest execution flaws and the best design
to represent effects of the intervention.
A median was calculated as a summary effect measure for each outcome of interest. For bodies of evidence consisting of
seven or more studies, an interquartile range was calculated as an index of variability. Unless otherwise noted, the results of each study were represented as a point estimate for the relative change in the violent outcome rate associated with the intervention.
The body of evidence of effectiveness was characterized as strong, sufficient, or insufficient on the basis of the number of available studies, the suitability of study designs for evaluating effectiveness, the quality of execution of the studies, the consistency of the results, and the median effect size
(12).
The Community Guide uses systematic reviews to evaluate the evidence of intervention effectiveness, and the Task Force makes recommendations based on the findings of these
reviews. The strength of each recommendation is based on the
strength of the evidence of effectiveness (i.e., the Task Force can recommend an intervention [or recommend against its use] on the basis of strong evidence of effectiveness or sufficient evidence of effectiveness**
[12]). Other types of evidence can also affect
a recommendation. For example, evidence that harms from an intervention outweigh improved outcomes might lead to
a recommendation against use of the intervention. If interventions are found to be effective, they are evaluated for
cost effectiveness by using economic evaluation guidelines developed for the
Community Guide (15). Because none of the
firearm laws reviewed was found to have sufficient evidence to draw conclusions regarding their effectiveness, no economic
reviews were conducted.
A finding of insufficient evidence to determine effectiveness should not be interpreted as evidence of ineffectiveness
but rather as an indicator that additional research is needed before an intervention can be evaluated for its effectiveness.
Results
The systematic review development team identified 51 studies that evaluated the effects of selected firearms laws on violence and met the inclusion criteria for this review. No study was excluded because of limitations in design or execution.
Information on violent outcomes was available in 48 studies, and the remaining three studies, which provided information on counts or proportions of regulated firearms used in crime, were used as supplementary evidence. Several studies examined more than
one type of firearm law.
Several separate studies evaluated effects of the same law in the same populations during overlapping time periods.
Such studies were considered nonindependent, and effect estimates from the best study in the group (as determined by the quality
of design and execution and the length of the follow-up
period) were chosen to represent the effects of the intervention. The
total number of studies for each intervention, and the number of studies that actually contributed effect estimates to the body
of evidence, are listed (Table). More extensive evidence
tables will be available at
http://www.thecommunityguide.org when the full evidence review is published.
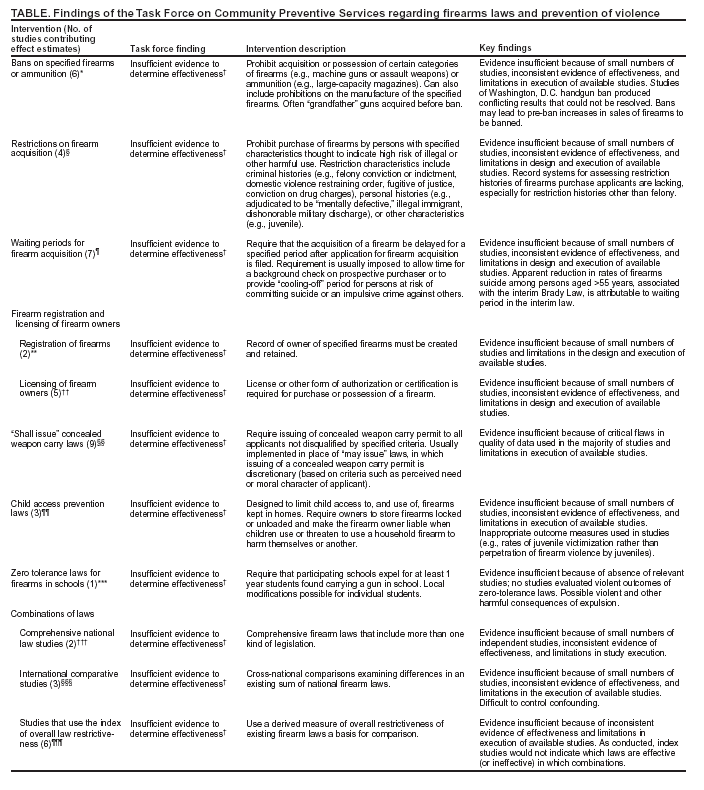
Evidence was insufficient to determine the effectiveness of any of these laws for the following reasons.
Bans on specified firearms or
ammunition. Results of studies of firearms and ammunition bans were
inconsistent: certain studies indicated decreases in violence associated with bans, and others indicated increases. Several studies found that the number of banned guns retrieved after a crime declined when bans were enacted, but these studies did not
assess violent consequences (16,17). Studies of the 1976 Washington, D.C. handgun ban yielded inconsistent results
(18--20). Bans often include "grandfather" provisions, allowing ownership of an item if it is acquired before the ban, complicating an assessment of causality. Finally, evidence indicated that sales of firearms to be
banned might increase in the period before implementation of the bans (e.g., the Assault Weapons Ban of
1994) (21).
Restrictions on firearm
acquisition. The federal government and individual states restrict the acquisition and use
of firearms by individuals on the basis of their personal history. Reasons for restriction can include prior felony
conviction, conviction of misdemeanor intimate partner violence, drug abuse, adjudication as "mentally
defective,"†† and other characteristics (e.g., specified young age). The Brady Law
(22) established national restrictions on acquisition of
firearms and ammunition from federal firearms licensees. The interim Brady Law (1994--1998) mandated a 5-day waiting period
to allow background checks. The permanent Brady Law, enacted in 1998, eliminated the required waiting period. It
normally allows 3 days for a background check, after which, if no evidence of a prohibited characteristic is found, the purchase may proceed (23). Certain states have established additional restrictions,
and some require background checks of all firearms transactions, not only those conducted by federal firearms licensees.
The permanent Brady Law depends on the National Instant Criminal Background Check System (NICS).
However, NICS lacks much of the required background information, particularly on certain restriction categories
(23). Efforts to improve the availability of background information have been supported by the National Criminal History Improvement Program (24). Approximately 689,000 applications to acquire a firearm (2.3% of 30 million applications) were denied under the Brady Law from its first implementation in 1994 through 2000
(25); the majority of denials were based on
the applicant's criminal history. However, denial of an application does not always stop applicants from acquiring
firearms through other means.
Overall, evaluations of the effects of acquisition restrictions on violent outcomes have produced inconsistent
findings: some studies indicated decreases in violence associated with restrictions, and others indicated increases. One
study indicated a statistically significant reduction in the rate of suicide by firearms among persons aged >55 years; however, the reduction in suicide by all methods was not statistically significant. Furthermore, this benefit appears to have been
a consequence of the waiting period imposed by the interim Brady Law (which has since been
dropped in the permanent law) rather than of the law's restrictions on the basis of the purchaser's characteristics
(26).
Waiting periods for firearm
acquisition. Waiting periods for firearm acquisition require a specified
delay between application for and acquisition of a firearm. Waiting periods have been established by the federal government
and by states to allow time to check the applicant's background or to provide a "cooling-off" period for persons at risk of committing suicide or impulsive acts against others. Studies of the effects of waiting periods on violent outcomes
yielded inconsistent results: some indicated a decrease in violent outcome associated with the delay and others indicated an increase. As noted previously, one study of the interim Brady Law indicated a statistically significant reduction in firearms suicide among persons aged >55 years associated with the waiting period requirement of the interim law. Several
studies suggested a partial "substitution effect" for suicide (i.e., decreases in firearms suicide are accompanied by smaller increases in suicide by other means) (26).
Firearm registration and licensing of
owners. Registration requires that a record of the owner of specified firearms
be created and retained (27). At the national level, the Firearm Ownership Protection Act of 1986 specifically precludes the federal government from establishing and maintaining a registry of firearms and their owners. Licensing requires
an individual to obtain a license or other form of authorization or certification to purchase or possess a firearm
(27). Licensing and registration requirements are often combined with other firearms regulations, such as safety training or safe storage requirements. Only four studies examined the effects of registration and licensing on violent outcomes; the findings
were inconsistent.
"Shall issue" concealed weapon carry
laws. Shall issue concealed weapon carry laws (shall issue laws) require the
issuing of a concealed weapon carry permit to all applicants not disqualified by specified criteria. Shall issue laws are
usually implemented in place of "may issue" laws, in which the issuing of a concealed weapon carry permit is discretionary (based on criteria such as the perceived need or moral character of the applicant). A third alternative, total prohibition of
the carrying of concealed weapons, was in effect in six states in 2001.
The substantial number of studies of shall issue laws largely derives from and responds to one landmark study (28). Many of these studies were considered to be nonindependent because they assessed the same intervention in the same population during similar time periods. A review of the data revealed critical problems, including misclassification of laws, unreliable county-level crime data, and failure to use appropriate denominators for the available numerator crime
data (29). Methodological problems, such as failure to adjust for autocorrelation
in time series data, were also evident. Results across studies were inconsistent or conceptually implausible. Therefore, evidence was insufficient to determine the effect
of shall issue laws on violent outcomes.
Child access prevention laws. Child access prevention (CAP) laws are designed to limit children's access to and use of firearms in homes. The laws require firearms owners to store their firearms locked, unloaded, or both, and make
the firearm owners liable when children use a household firearm to threaten or harm themselves or others. In three states
with CAP laws (Florida, Connecticut, California), this crime is a felony; in several others it is a misdemeanor.
Only three studies examined the effects of CAP laws on violent outcomes, and only one outcome, unintentional
firearms deaths, was assessed by all three. Of these, two studies assessed the same states over the same time periods and were therefore nonindependent. The most recent study, which included the most recent states to pass CAP laws and had
the longest follow-up time, indicated that the apparent reduction in unintentional firearm deaths associated with CAP laws that carry felony sanctions was statistically significant only in Florida and not in California or Connecticut
(30). Overall, too few studies of CAP law effects have been done, and the findings of existing studies were inconsistent. In addition, although CAP laws address juveniles as perpetrators of firearms violence, available studies assessed only juvenile victims of firearms violence.
Zero tolerance laws for firearms in
schools. The Gun-Free Schools Act (31) stipulates that each state receiving
federal funds must have a state law requiring local educational agencies to expel a student from school for at least 1 year if
a firearm is found in the student's possession at school. Expulsion may lead to alternative school placement or to
"street" placement (full expulsion, with no linkage to formal education). In contrast to the 3,523 firearms reported confiscated under the Gun-Free Schools Act in the 1998--99 school year, school surveys
(32) indicate that an estimated 3% of the
12th grade student population in 1996 (i.e., 85,350 students) reported carrying firearms on school property one or more
times in the previous 30 days. Thus, even if only 12th grade students carry firearms, fewer than 4.3% of firearms are
being detected in association with the Gun-Free Schools Act.
No study reviewed attempted to evaluate the effects of zero tolerance laws on violence in schools, nor did any
measure the effect of the Gun-Free Schools Act on carrying of firearms in schools. One cross-sectional study, however, assessed
the effectiveness of metal detector programs in reducing the carrying of firearms in schools
(33). Although firearms detection is not explicitly required in the Gun-Free Schools Act, the effectiveness of the law may depend on the ability to detect firearms by various means. The study reported that schools with and without metal detectors did not differ in rates
of threatening, fights, or carrying of firearms outside of school, but the rate of carrying firearms to, from, or in schools
with detection programs was half that of schools without such programs. The effectiveness of zero tolerance laws in
preventing violence cannot be assessed because appropriate evidence was not available. A further concern is that "street" expulsion might result in increased violence and other problems among expelled students.
Combinations of firearms laws. Governmental jurisdictions (e.g., states or nations) can be characterized by the degree to which they regulate firearm possession and use. Whether a greater degree of firearms regulation in a jurisdiction results in
a reduction of the amount of violence in that jurisdiction still needs to be determined. Three kinds of evidence were
reviewed for this study: 1) studies of the effects of comprehensive national laws within nations;
2) international comparisons of comprehensive laws; and 3) studies in which law types within jurisdictions (i.e., regulation of specific, defined aspects of firearm acquisition and use) were categorized and counted, and counts compared with rates of specific forms of
violence within the same jurisdictions. The latter type are referred to here as index studies because they developed indices of the
degree of regulation. In drawing conclusions about law combinations, findings from the three approaches were considered.
On the basis of national law assessments (the Gun Control Act of 1968 in the United States and the Criminal
Law Amendment Act of 1977 in Canada), international comparisons (between the United States and Canada), and
index studies (all conducted within the United States), available evidence was insufficient to determine whether the degree of firearms regulation was associated with decreased
(or increased) violence. The findings were inconsistent
and most studies were methodologically inadequate to allow conclusions about causal effects. Moreover, as conducted, index studies, even if consistent, would not allow specification of which laws to implement.
In summary, the Task Force found insufficient evidence to determine the effectiveness of any of the firearms laws reviewed
for preventing violence. References and key findings are listed (Table).
Research Needs
The Task Force's review of firearms laws found insufficient evidence to determine whether the laws reviewed
reduce (or increase) specific violent outcomes (Table). Much existing research suffers from problems with data, analytic methods,
or both. Further high-quality research is required to establish the relationship between firearms laws and violent
outcomes. Potential areas for further investigation will be discussed in detail in an upcoming article in the
American Journal of Preventive Medicine.
Several recurring problems were associated with the studies that evaluated the effects of firearms laws on violent outcomes:
The assessment or "measurement" of laws and their provisions has been noted as a problem in certain studies and may occur in others as well. As with all interventions,
assessing the degree of implementation of laws may be important
in evaluating their effects; yet this has not been a part of law evaluations. Better information regarding implementation
might allow more sophisticated explanation of inconsistent effects.
Several facets of the measurement of violent outcomes have been problematic. Crime data are substantially
underreported and, at the county level, may not be sufficiently reliable for research purposes
(29). In addition, selected outcome
measures are often not directly relevant to the law being assessed (e.g., the evaluation of child
access prevention laws by measurement of juvenile victims [rather than perpetrators] and the evaluation of shall issue laws by the measurement of crimes occurring in the home [where the law does not apply]). Another problem is that crime data are often aggregated, so that
the circumstances of violent events cannot be determined. Aggregated data hinder the assessment of the ways in which
laws might and might not work. Individual record data systems currently being implemented --- the National
Incident-Based Reporting System of the FBI and the
National Violent Death Reporting System of CDC and partners --- might
resolve some of these difficulties and greatly facilitate the evaluation of firearms laws.
The measurement of potential confounders has been a challenge in evaluating the effects of firearms laws. Potentially important confounders include socioeconomic status and poverty, drug cycles, gang activity, and the intensity of law enforcement. Measuring these phenomena is difficult and requisite data are often not available. In addition, endogeneity (i.e., the presence of common characteristics, such as crime counts, as both dependent and independent variables in equations) has been a problem in firearms law evaluations.
Study designs and analytic techniques used in firearms law evaluations have been problematic. Rates of violence may affect the passage of firearms laws and firearms laws may then affect rates of violence; knowledge of temporal sequence is
thus critical in separating cause and effect, and cross-sectional studies are at a disadvantage. Time series analyses of firearms laws and violent outcomes have not consistently adjusted for temporal and spatial autocorrelation, and thus may
have exaggerated hypothesized associations. Additionally, firearms studies often fail to note potential biases associated
with measurement of outcomes not directly associated with the law in question (e.g., using victims rather than agents of violence in the assessment of CAP laws).
In conclusion, the application of imperfect methods to
imperfect data has commonly resulted in inconsistent and otherwise insufficient evidence with which to determine the effectiveness of firearms laws in modifying violent outcomes.
This is a critical period for focused research on the effectiveness of firearms laws in reducing violence in the United States. International comparisons indicate that the United States is an outlier among developed, industrialized nations in rates
of firearms violence (2). Widespread public concern exists about criminal firearms violence, firearms violence among youth, and other forms of firearms violence, and popular support for many firearms laws is evident
(34,35). Although the Task Force's systematic review of the existing literature on firearms laws found insufficient evidence to determine the effectiveness of these laws in preventing violence, research should continue on the effectiveness of firearms laws as one approach to the prevention
or reduction of firearms violence and firearms injury. Evaluation should include not only the laws reviewed here, but the
broad array of other federal, state, and local laws.
Additional Information Regarding the
Community Guide
In addition to the firearms laws reviewed in this report,
reviews for the Community Guide have been completed on
the effectiveness of preventing violence through early childhood home visitation
(36) and therapeutic foster care (to be published
in the near future). Reviews of several other violence prevention interventions are pending or under way, including the effects of school-based, social and emotional skill learning programs, and the treatment of juveniles as adults in the justice system.
Community Guide topics are prepared and released as each is completed. The findings from systematic reviews on vaccine-preventable diseases, tobacco use prevention and reduction, motor vehicle occupant injury, physical activity, diabetes, oral health, and the social environment have been published. A compilation of systematic reviews will be published in book form
in 2004. Additional information regarding the Task Force, the Community Guide, and a list of published articles is available at
http://www.thecommunityguide.org.
References
Miniño AM, Arias E, Kochanek KD, Murphy SL, Smith BL. Deaths: final data for 2000. Hyattsville, MD: US Department of Health and
Human Services, CDC, National Center for Health Statistics,
2002. (National vital statistics reports; vol. 50, no. 15). Available at
http://www.cdc.gov/nchs/data/nvsr/nvsr50/nvsr50_15.pdf.
Bureau of Justice Statistics. Sourcebook of criminal justice statistics 2000. Washington, DC: US Department of Justice, Bureau of Justice
Statistics, 2001.
Krug EG, Powell KE, Dahlberg LL. Firearm-related deaths in the United States and 35 other high- and upper-middle-income countries. Int
J Epidemiol 1998;27:214--21.
Cook PJ, Lawrence BA, Bruce A, Ludwig J, Miller TR. The medical costs of gunshot injuries in the United States. JAMA 1999;282:447--54.
Bureau of Alcohol Tobacco and Firearms. Commerce in firearms in the United States. Washington, DC: US Department of the Treasury,
Bureau of Alcohol, Tobacco and Firearms, 2000.
Cook PJ, Ludwig J. Guns in America: results of a comprehensive
national survey on firearms ownership and use. Washington, DC: US Department
of Justice, National Institute of Justice, 1996.
Schuster MA, Franke TM, Bastian AM, Sor S, Halfon N. Firearm storage patterns in US homes with children. Am J Public Health 2000;90:588--94.
Cukier W. Firearms regulation: Canada in the international context. Chronic Dis Can 1998;19:25--34.
Kellermann AL, Lee RK, Mercy JA, Banton JG. The epidemiologic basis for the prevention of firearm injuries. Annu Rev Public Health
1991;12:17--40.
Powell EC, Sheehan KM, Christoffel KK. Firearm violence among youth: public health strategies for prevention. Ann Emerg Med 1996;28:204--12.
Briss PA, Zaza S, Pappaioanou M, et al. Developing an evidence-based Guide to Community Preventive Services---methods. Am J Prev
Med 2000;18(1S):35--43.
US Department of Health and Human Services. Healthy people 2010. 2nd ed. With Understanding and Improving Health and Objectives
for Improving Health (2 vols). Washington, DC: US Department of Health and Human Services, 2000.
Zaza S, Wright-de Aguero LK, Briss PA, et al. Data collection instrument and procedure for systematic reviews in the Guide to Community
Preventive Services. Am J Prev Med 2000;18(1S):44--74.
Carande-Kulis VG, Maciosek MV, Briss PA, et al. Methods for systematic reviews of economic evaluations for the Guide to Community
Preventive Services. Am J Prev Med 2000;18(1S):75--91.
Weil DS, Knox RC. The Maryland ban on the sale of assault pistols and high-capacity magazines: estimating the impact in Baltimore. Am J
Public Health 1997;87:297--8.
Vernick JS, Webster DW, Hepburn LM. Effects of Maryland's law banning Saturday night special handguns on crime guns. Inj Prev 999;5:259--63.
Loftin C, McDowall D, Wiersma B, Cottey TJ. Effects of restrictive licensing of handguns on homicide and suicide in the District of
Columbia. N Engl J Med 1991;325:1615--20.
Britt CL, Bordua DJ, Kleck G. A reassessment of the D.C. gun law: some cautionary notes on the use of interrupted time series designs for
policy impact assessment. Law Soc Rev 1996;30:361--80.
McDowall D, Wiersma B, Loftin C. Using quasi-experiments to evaluate firearm laws: comment on Britt et al.'s reassessment of the D.C. gun law.
Law Soc Rev 1996;30:381--91.
Roth JA, Koper CS. Impacts of the 1994 Assault Weapons Ban: 1994--996. Washington, DC: US Department of Justice, National Institute of
Justice, 1999.
Public Law 103-159. Brady Handgun Violence Prevention Act, 18 USC, Section 922(t).1995.
US General Accounting Office. Gun control: options for improving the National Instant Criminal Background Check System. Washington, DC:
US General Accounting Office, Report to Congressional
Requesters, April 2000. GAO/GGD-00-56
US Department of Justice. Improving criminal history records for background checks. Bureau of Justice Statistics Highlights. Washington, DC:
US Department of Justice, February 11, 2002.
Bowling M, Lauver G, Gifford SL, Adams DB. Background checks for firearm transfers, 2000. Bureau of Justice Statistics Bulletin. Washington,
DC: US Department of Justice, July 2001.
Ludwig J, Cook PJ. Homicide and suicide rates associated with implementation of the Brady Handgun Violence Prevention Act. JAMA
2000;284:585--91.
DeFrancesco S, Vernick JS, Weitzel MM, LeBrun EE. A gun policy glossary: policy, legal and health terms. Baltimore, MD: The Johns Hopkins
Center for Gun Policy and Research, 2000.
Maltz MD, Targonski J. A note on the use of county-level UCR data.
J Quant Criminol 2002;18:297--318.
Webster DW, Starnes M. Reexamining the association between child access prevention gun laws and unintentional shooting deaths of
children. Pediatrics 2000;106:1466--9.
Public Law 103-382. Improving America's Schools Act of 1994. 20 USC 8921, Section 14601, Gun-Free Schools Act, 1994.
US Department of Education and US Department of Justice. 1999 Annual report on school safety. Washington, DC: U.S. Department of
Education and US Department of Justice, 1999. Available at
http://www.ed.gov/PDFDocs/InterimAR.pdf
Ginsberg C. Violence-related attitudes and behaviors of high school students---New York City, 1992. J Sch Health 1993;63:438--40.
* A firearm is a weapon (e.g., a handgun, rifle, or shotgun) in which a shot is propelled by gunpowder.
† Consultants for the systematic reviews of violence prevention interventions were Laurie Anderson, Ph.D., CDC, Olympia, Washington; Carl Bell, M.D., Community Mental Health Council, Chicago, Illinois; Red Crowley, Men Stopping Violence, Atlanta, Georgia; Sujata Desai, Ph.D., CDC, Atlanta,
Georgia; Deborah French, Colorado Department of Public Health and Environment, Denver, Colorado; Darnell F. Hawkins, Ph.D., J.D., University of Illinois at Chicago, Chicago, Illinois; Danielle LaRaque, M.D., Harlem Hospital Center, New York, New York; Barbara Maciak, Ph.D., CDC, Detroit, Michigan;
James Mercy, Ph.D., CDC, Atlanta, Georgia; Suzanne Salzinger, Ph.D., New York State Psychiatric Institute, New York, New York; Patricia Smith, M.S.,
Michigan Department of Community Health, Lansing, Michigan. Other aspects of this review benefited by comments from Phillip Cook, Ph.D., Duke
University, Durham, North Carolina; Gary Kleck, Ph.D., School of Criminology and Criminal Justice, Florida State University, Tallahassee, Florida; Jon Vernick, Ph.D., Johns Hopkins University, Baltimore, Maryland; Daniel Webster, Sc.D., Johns Hopkins University, Baltimore, Maryland; James Wright, Ph.D., University
of Central Florida, Orlando, Florida; Frank Zimring, J.D., University of California, Berkeley, California.
§ Established Market Economies as defined by the World Bank are Andorra, Australia, Austria, Belgium, Bermuda, Canada, Channel Islands, Denmark, Faeroe Islands, Finland, France, Germany, Gibraltar, Greece, Greenland, Holy See, Iceland, Ireland, Isle of Man, Italy, Japan, Liechtenstein, Luxembourg, Monaco,
the Netherlands, New Zealand, Norway, Portugal, San Marino, Spain, St. Pierre and Miquelon, Sweden, Switzerland, the United Kingdom, and the United States.
** At the June 2002 meeting of the Task Force on Community Preventive Services, new terminology was adopted to reflect the findings of the Task Force. Instead
of being referred to as "strongly recommended" and "recommended," such interventions are now referred to as "recommended (strong evidence of effectiveness)" and "recommended (sufficient evidence of effectiveness)," respectively. Similarly, the finding previously referred to as "insufficient evidence" is now more fully stated: "insufficient evidence to determine effectiveness." These changes were made to improve the clarity and the intent of the findings.
†† The term "mentally defective" is a determination by a lawful authority that a person, as a result of marked subnormal intelligence or mental illness, is a danger to self or others, or lacks the mental capacity to manage his or her own affairs. The term also includes a court finding of insanity in a criminal case, incompetence
to stand trial, or not guilty by reason of lack of mental responsibility.
Source: Bureau of Alcohol Tobacco and Firearms. Federal firearms regulations reference
guide. Washington, DC: U.S. Department of the Treasury, Bureau of Alcohol, Tobacco and Firearms, 2000, ATF P 5300.4 (01-00). Available at
http://www.atf.treas.gov/pub/fire-explo_pub/2000_ref.htm.
Task Force on Community Preventive Services*
November 1, 2002
Chair:
Jonathan E.
Fielding, M.D., Los Angeles Department of Health Services, Los Angeles,
California
Vice-Chair:
Patricia Dolan
Mullen, Dr.P.H., University of Texas-Houston School of Public Health,
Houston, Texas
Members: Ross C. Brownson,
Ph.D., St. Louis University School of Public Health, St. Louis, Missouri;
John Clymer, Partnership for Prevention, Washington, D.C.; Jane L.
Delgado, Ph.D., National Alliance for Hispanic Health, Washington, D.C.;
Mindy Thompson Fullilove, M.D., New York State Psychiatric Institute and
Columbia University, New York, New York; Alan R. Hinman, M.D., Task Force
for Child Survival and Development, Atlanta, Georgia; George J. Isham,
M.D., HealthPartners, Minneapolis, Minnesota; Garland H. Land, M.P.H.,
Center for Health Information Management and Epidemiology, Missouri
Department of Health, Jefferson City, Missouri; Patricia A. Nolan, M.D.,
Rhode Island Department of Health, Providence, Rhode Island; Dennis E.
Richling, M.D., Union Pacific Railroad, Omaha, Nebraska; Susan C.
Scrimshaw, Ph.D., School of Public Health, University of Illinois,
Chicago, Illinois; Steven M. Teutsch, M.D., Merck & Company, Inc., West
Point, Pennsylvania; Robert S. Thompson, M.D., Department of Preventive
Care, Group Health Cooperative of Puget Sound, Seattle, Washington
Consultants: Robert S.
Lawrence, M.D., Bloomberg School of Public Health, Johns Hopkins
University, Baltimore, Maryland; J. Michael McGinnis, M.D., Robert Wood
Johnson Foundation, Princeton, New Jersey; Lloyd F. Novick, M.D., Onondaga
County Department of Health, Syracuse, New York
* Patricia A. Buffler, Ph.D., University of California,
Berkeley; Mary Jane England, M.D., Regis College, Weston, Massachusetts;
Caswell A. Evans, Jr., D.D.S., National Oral Health Initiative, Office of
the U.S. Surgeon General, Rockville, Maryland; David W. Fleming, M.D.,
CDC, Atlanta, Georgia; Fernando A. Guerra, M.D., San Antonio Metropolitan
Health District, San Antonio, Texas; and Charles S. Mahan, M.D., College
of Public Health, University of South Florida, Tampa, Florida, also served
on the Task Force while the recommendations were being developed.
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services.References to non-CDC sites on the Internet are
provided as a service to MMWR readers and do not constitute or imply
endorsement of these organizations or their programs by CDC or the U.S.
Department of Health and Human Services. CDC is not responsible for the content
of pages found at these sites. URL addresses listed in MMWR were current as of
the date of publication.
All MMWR HTML versions of articles are electronic conversions from ASCII text
into HTML. This conversion may have resulted in character translation or format errors in the HTML version.
Users should not rely on this HTML document, but are referred to the electronic PDF version and/or
the original MMWR paper copy for the official text, figures, and tables.
An original paper copy of this issue can be obtained from the Superintendent of Documents,
U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800.
Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to
mmwrq@cdc.gov.