|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
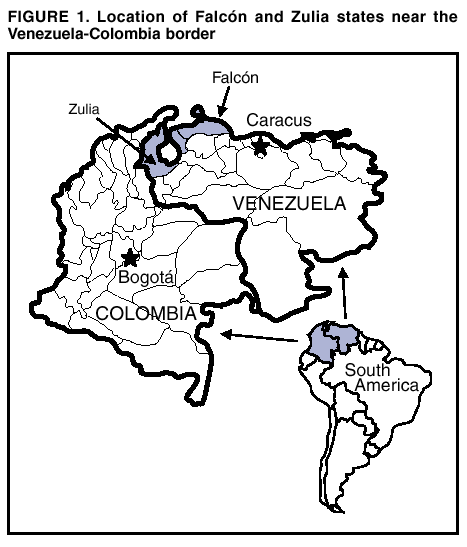
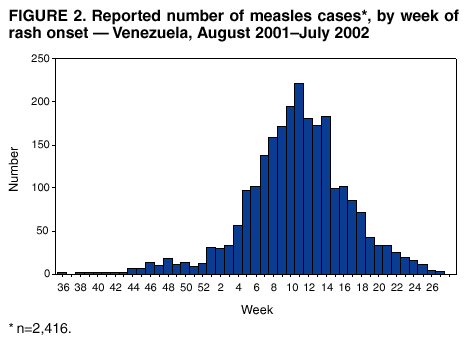
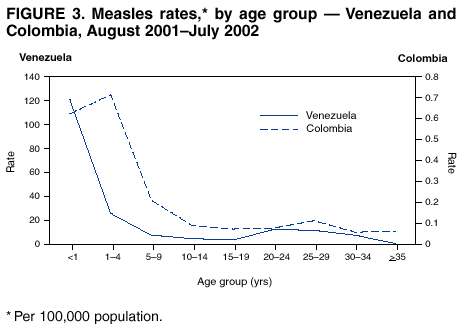
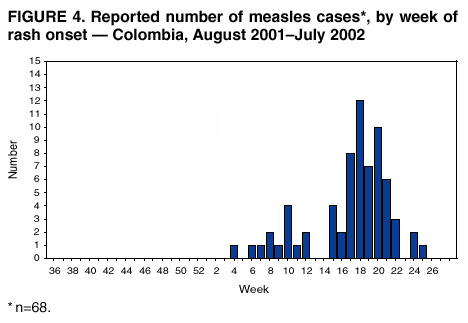
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Outbreak of Measles --- Venezuela and Colombia, 2001--2002Substantial progress has been made toward interrupting indigenous measles transmission in the Region of the Americas (1--4). In 2001, the number of confirmed measles cases in the region reached a record low of 537 cases, a 99% decrease since 1990 (4). During 2001, the Dominican Republic and Haiti interrupted indigenous measles transmission successfully (4,5), ending known indigenous transmission of the D6 measles virus genotype. This genotype, which had circulated widely in the Region of the Americas since 1995, caused nationwide outbreaks in Argentina, Bolivia, Brazil, the Dominican Republic, and Haiti during 1997--2001 (3--7). In August 2001, a measles outbreak introduced by a traveler returning from Europe occurred in Venezuela and was exported to Colombia in 2002. This report describes the epidemiology of the outbreaks and control measures implemented by the ministries of health of Venezuela and Colombia. VenezuelaIn 2000, measles vaccination coverage in Venezuela was 84% on the basis of administrative data reported routinely. By September 2001, estimated coverage had decreased to 58% and was lower in Venezuelan states near the border with northern Colombia (e.g., Falcón, 44%; Zulia, 34%) (Figure 1). During 2001--2002, two outbreaks of measles occurred in Venezuela. On August 29, 2001, a man aged 39 years (index case) had rash onset of measles 1 day before returning to Falcón from a trip to Switzerland, Germany, and Spain during August 4--30. Approximately 1 month later, an investigation was initiated by local health authorities to identify additional cases. The first laboratory-confirmed case was reported on September 28 and occurred in the index patient's brother, aged 35 years, who had rash onset on September 23. The majority of persons who were affected by the outbreak were health-care workers, laborers, and students. The outbreak lasted until December 15, affected 37 persons in three municipalities, and ended after implementation of a statewide vaccination campaign for children aged 1--14 years. In January 2002, a second outbreak of measles was introduced into Falcón from Zulia by a girl aged 7 months who had visited a tourist site in Falcón and who had received medical care at a local hospital. She infected a nurse, who then transmitted the disease to other persons. Of 165 persons reported from Falcón during this outbreak, 85 (52%) had visited the same tourist site. The first confirmed measles case in Zulia occurred in a woman aged 27 years who was an auxiliary nurse in a physician's office that provided care to residents of Falcón. The nurse had onset of rash on October 25, 2001, and subsequently infected four other persons. During the next 3 months, the outbreak spread to all municipalities in Zulia; 2,074 cases had been confirmed as of July 24, 2002. For several chains of transmission, the index case occurred in a health-care worker. Beginning in February 2002, the outbreak spread to 14 additional states in Venezuela, including four states bordering Colombia. During October 2001--July 2002, Venezuela reported 6,380 suspected measles cases; of these, 2,416 were laboratory or epidemiologically confirmed.* The outbreak peaked during the week of March 16 (week 11) (Figure 2) and has affected 16 (67%) of the 24 states in Venezuela. A total of 2,074 (86%) cases were from Zulia, 202 (8%) from Falcón, and 140 (4%) from the other 14 states. The age groups most affected were children aged <1 year (120 cases per 100,000 population), children aged 1--4 years (26), and persons aged 20--24 years (12) (Figure 3). During November 2001--January 2002, measles virus samples were collected from patients in Zulia. Genetic sequencing indicated that the virus was not similar to viruses encountered previously in the region or to the reference genotype strains available on the measles sequence database. A close match was identified from virus samples taken from cases imported into Australia from Indonesia as early as 1999, which have been given the proposed designation of genotype d9† (D. Chibo, Ph.D., World Health Organization, Measles Reference Laboratory [Western Pacific Region], Australia, personal communication, 2002). During November 2001--January 2002, a follow-up measles vaccination campaign was implemented targeting approximately 2.2 million children aged 1--4 years; 16 of the 24 states reported coverage of 100%. However, the outbreak continued with cases occurring in all age groups. House-to-house monitoring of vaccination coverage revealed areas with unvaccinated children. In March 2002, a nationwide vaccination campaign was implemented targeting approximately 5.5 million children aged 6 months--14 years and an estimated 5.5 million adults at high risk (e.g., health-care workers, tourists, factory workers, soldiers, university students, and migrants) in urban, periurban (densely populated informal settlements), and rural areas. Vaccination coverage among adults at high risk in that campaign was estimated to be 76% as of July 6 (week 27). ColombiaColombia shares a border with Venezuela, with which it has substantial commerce and migration in Zulia. In 1996, measles vaccination coverage for children in Colombia was 94%. In 2000, measles coverage for children aged 1 year declined to 80%. Coverage for children aged 1 year increased to 91% during 2001. In January 2002, the first confirmed case occurred in a girl aged 7 years from Colombia. She had rash onset on January 20 and reported previous contact in Zulia with persons with confirmed measles. As of July 6 (week 27), 68 cases have been confirmed (Figure 4). Confirmed cases have occurred in 19 municipalities in 10 (30%) of the 33 departments; 17 affected municipalities were located on the Atlantic coast and/or bordered Venezuela. As of July 18, the most recent confirmed patient had rash onset on July 17 (week 29). Of the 68 confirmed cases, 18 (26%) were imported from Venezuela, 35 (51%) were epidemiologically linked to those importations, nine (13%) were from unknown sources, and six (9%) are under investigation. Of 44 patients aged 1--4 years, 15 (34%) had received measles vaccine previously. The age groups most affected were children aged <5 years (0.7 per 100,000 population), children aged 5--9 years (0.2), and persons aged 25--29 years (0.1) (Figure 3). Control activities being implemented include 1) door-to-door measles vaccination campaigns in high-risk municipalities as part of a national vaccination campaign for approximately 3.8 million children aged 6 months--5 years and other adults at high risk (e.g., health-care workers, migrants, and travelers), 2) house-to-house vaccination coverage monitoring in areas at high risk, 3) strengthening of national measles surveillance, and 4) increased training in case investigation and outbreak control. As of July 10, 2002, a total of 2,587,408 (73%) children in the target group had been vaccinated. During these outbreaks, measles surveillance has been heightened by using active case searches in both countries, with 2,198 suspected cases detected (5.4 per 100,000 population) in Colombia and 6,380 (26.5) in Venezuela. Technical and financial resources have been provided by international organizations, including Pan American Health Organization, United Nations Children's Fund (UNICEF), and CDC. Reported by: H Izurieta, M Brana, P Carrasco, V Dietz, G Tambini, CA de Quadros, Div of Vaccines and Immunizations; Pan American Health Organization, Washington, DC. O Barrezueta, Pan American Health Organization; N López, D Rivera, L López, M Villegas, E Maita, Ministry of Health; C Garcia, National Institute of Hygiene, Caracas, Venezuela. D Pastor, Pan American Health Organization; C Castro, J Boshell, O Castillo, G Rey, F de la Hoz, D Caceres, M Velandia, National Institute of Health, Ministry of Health, Bogotá, Colombia. W Bellini, J Rota, P Rota, Div of Viral and Rickettsial Diseases, National Center for Infectious Diseases; F Lievano, C Lee, Global Immunization Div, National Immunization Program, CDC. Editorial Note:The reintroduction of measles and its subsequent transmission in Venezuela and exportation to Colombia indicates that, until global measles eradication is achieved, countries in the Region of the Americas are vulnerable to importations. However, these importations should not result in sustained measles transmission if vaccination coverage is maintained at high levels (>95%) in all municipalities and follow-up campaigns are conducted on time (3,4). Low vaccination coverage in Venezuela and deficiencies in surveillance contributed to the outbreak. The first report of a case was delayed for approximately 1 month, sufficient time for the occurrence of several generations of transmission and spread to other areas. Colombia initiated aggressive vaccination activities in 2001 when Venezuela began reporting cases. The limited transmission in Colombia suggests that efforts to prevent a large outbreak might have been successful. However, because of civil conflict in several areas, confirming the lack of virus transmission was difficult. In addition, a contributing factor to lower transmission in Colombia might have been the higher measles coverage rates before the outbreak compared with Venezuela. Measures to control measles outbreaks in the Region of the Americas include 1) partnerships with local governments to secure financial and logistical resources, 2) rapid identification and vaccination of groups at high risk (e.g., health-care workers, migrants, and tourist industry personnel), 3) house-to-house monitoring of vaccination coverage, 4) expansion of the target group to older ages if incidence is high in these age cohorts, and 5) heightened surveillance in all regions of the country. References
* Epidemiologically linked to another laboratory-confirmed measles case.
Figure 1
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 8/29/2002 |
|||||||||
This page last reviewed 8/29/2002
|