|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
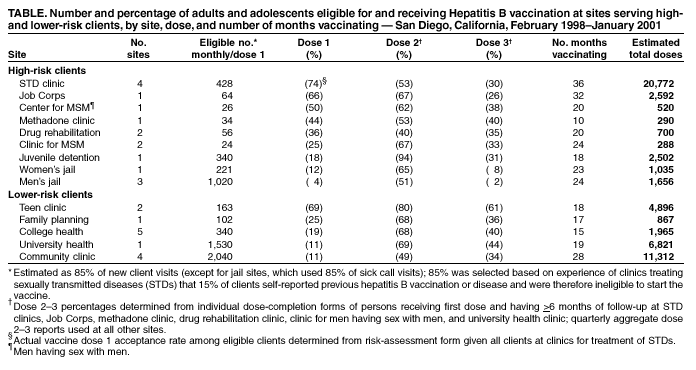
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Hepatitis B Vaccination Among High-Risk Adolescents and Adults --- San Diego, California, 1998--2001The national strategy to eliminate hepatitis B virus (HBV) transmission is based on 1) screening all pregnant women for hepatitis B surface antigen and post-exposure vaccination of infants of infected mothers; 2) vaccinating all infants as part of the childhood vaccination schedule; 3) vaccinating children and adolescents not vaccinated previously; and 4) vaccinating adolescents and adults in groups at increased risk for infection (1,2). These strategies have been implemented successfully in the United States except for the vaccination of adults and older adolescents at high risk (2). This report describes the initial findings of a hepatitis B vaccination program for potentially high-risk adolescents and adults conducted in areas of San Diego County, California. The findings indicate that high rates of hepatitis B vaccination can be achieved in clinics and programs that serve persons at high risk for HBV infection through the integration of hepatitis B vaccination into routine preventive health-care services. Improved efforts to vaccinate adolescents and adults at increased risk for HBV infection are critical to reduce disease incidence and prevent chronic HBV infection. The San Diego Viral Hepatitis Prevention Project (VHPP) began in February 1998 with the selection of a convenience sample of sites* located primarily in the central and southeast areas of San Diego County, where the incidences of gonorrhea and chlamydia are higher than in other parts of the county. The population of San Diego County is approximately 2.9 million persons, and the population of the central and southeast areas is approximately 500,000 persons. Sites that serve both clients at high risk and those with a lower risk for HBV infection were selected. Hepatitis B vaccine was provided at no cost to participating sites, and project staff assisted site personnel in developing educational materials and administrative procedures and in monitoring vaccine coverage and completion. At sites that did not provide clinical services, the project provided a vaccination nurse on selected days. At all participating sites, clinic managers/program administrators agreed to offer vaccine to all clients without collecting client-specific risk information. At most sites, clients starting vaccination were asked to complete a self-administered sexually transmitted disease (STD)/hepatitis risk-assessment form that included information about previous hepatitis B vaccination or infection. All STD clinic clients were asked to complete the risk-assessment form to determine the percentage of clients eligible to start vaccination (i.e., those with no self-reported history of previous hepatitis B vaccination or infection). Approximately 85% of STD clients were eligible to start hepatitis B vaccination; this percentage was used at other project sites to estimate the number of eligible clients. Risk criteria were not used to determine eligibility. STD ClinicsHepatitis B vaccination was offered to all clients of the county health department's STD clinics. During February 1998--January 2001, risk-assessment forms were completed by 18,221 clients, of whom 1,900 (10%) reported previous completion of the hepatitis B vaccination series. Among men who have sex with men (MSM) and injection-drug users (IDUs), 16% (286 of 1,755) and 6% (67 of 1,106), respectively, reported having completed the vaccination series previously; among those aged <25 years, 12% (31 of 265) of MSM and 8% (12 of 153) of IDUs reported completion of the series. Of 18,221 clients completing risk-assessment forms, 15,502 (85%) were eligible to begin the vaccination series, of whom 11,405 (74%) received the first dose of vaccine. Of the 9,697 clients for whom >6 months had elapsed since they received the first dose, 5,123 (53%) received the second dose, and 2,910 (30%) completed the 3-dose series (Table). To improve vaccination acceptance rates, during October 1999--December 2000, the main clinic offered all clients a 5-minute counseling session about hepatitis B vaccination. The acceptance rate for the first dose increased from 66% (4,390 of 6,615) during February 1998--September 1999 (before counseling was initiated) to 77% (3,094 of 4,040) during the 15-month counseling period (rate ratio [RR]=1.15; 95% confidence interval [CI]=1.13--1.18; p<0.001). Because of staff shortages and scheduling difficulties, counselors were not available on all days; as a result, some clients were not counseled. Among the 1,861 clients counseled, the acceptance rate for the first dose was 80%, compared with 74% (1,610 of 2,189) for clients who were not counseled (RR=1.08; 95% CI=1.05--1.12; p<0.001). HIV counselors now provide hepatitis prevention and vaccination information as part of pretest HIV counseling offered to all clients. Other SitesOther sites serving primarily clients at high-risk attained first-dose vaccination coverage rates of 4%--66%, with correctional institutions (i.e., county juvenile detention and adult jail) and a health-care clinic serving MSM having the lowest first-dose coverage rates (Table). At sites serving primarily clients at lower-risk, vaccine coverage was <30% at all sites except teen clinics, which had a first-dose coverage rate of 69%. Although community primary-care clinics vaccinated the most clients each month, their first-dose vaccination coverage rate was 11%. Clinic managers had agreed to implement a policy of offering vaccination to all new eligible clients; however, some clinics might have offered vaccine selectively based on clinical judgment of risk or were unable to integrate vaccination into their regular schedules. Project support for hepatitis B vaccination continues at most high-risk sites. In addition, other viral hepatitis prevention services (e.g., selective hepatitis B and hepatitis C serologic screening, hepatitis A vaccination, and STD screening services) have been or are being integrated into STD clinics, court-ordered drug-offender rehabilitation programs, and anonymous HIV counseling and testing sites. The San Diego VHPP developed a guide for establishing hepatitis B vaccination services in an STD clinic (http://www.cdc.gov/hepatitis/spotlights/integration.htm). The guide has been distributed to all state health department STD, hepatitis C prevention, and vaccination programs. Reported by: P Murray, MPH, C Brennan, MPH, S O'Neill, MS, P Gonzales, R Gilchick, MD, Public Health Svcs, Health and Human Svcs Agency, San Diego County, California. Div of Viral Hepatitis, National Center for Infectious Diseases; R Gunn, MD, Div of Sexually Transmitted Diseases Prevention, National Center for HIV, STD and TB Prevention; D Callahan, MD, Div of Applied Epidemiology and Training, Epidemiology Program Office, CDC. Editorial Note:Data from the San Diego VHPP indicate that high rates of hepatitis B vaccination can be achieved in some clinics and programs that serve persons at high risk for HBV infection through the integration of hepatitis B vaccination into routine clinic and program services. In the United States, the incidence of reported cases of acute hepatitis B has declined 76% since the late 1980s (3). The greatest decline has occurred among persons aged 10--29 years, and the median age of persons with acute hepatitis B has increased approximately 5 years during the 1990s (3). Universal vaccination of infants and adolescents prevents HBV infections within these age groups and eventually will prevent transmission among adults. However, because it will take several decades to achieve the secondary benefit of hepatitis B vaccination of infants and young adolescents, vaccination of older adolescents and of adults at increased risk for HBV infection is needed to reduce disease incidence and chronic HBV infection prevalence in the near future (3). As with other vaccines recommended to prevent disease among older adolescents and adults, achieving high levels of hepatitis B vaccine coverage among these groups at increased risk for HBV infection has been difficult. Several obstacles account for low vaccine coverage including 1) inability of health-care providers to identify and deliver vaccine to at-risk populations; 2) lack of a public health infrastructure to support adult vaccination; 3) lack of familiarity by health-care providers with practices required to achieve high rates of adult vaccination; and 4) limited private- and public-sector reimbursement for adult vaccination. Many persons at increased risk for HBV infection are clients of programs that provide other prevention and clinical services, at times in nonclinical settings. The San Diego VHPP tested the feasibility of vaccinating adults and older adolescents at increased risk for HBV infection at sites that provide services to such persons. For example, hepatitis B vaccination is recommended for all persons seeking care at STD clinics, a setting that provides services to the greatest number of adults at increased risk for HBV infection. Among persons with acute hepatitis B reported annually to a CDC hepatitis surveillance system, approximately 35% have been treated previously for STDs, which indicates the importance of this setting in the prevention of HBV infections (3). Earlier attempts at hepatitis B vaccination in STD clinics had limited success; first-dose acceptance rates varied (range: 44%--70%), and <30% of persons completed the 3-dose series (4; CDC, unpublished data, 1993, 1997). By providing counseling as part of an integrated service, the San Diego VHPP was able to achieve first-dose acceptance rates as high as 80%. The goal of hepatitis B vaccination programs is to achieve the highest possible rate of 3-dose vaccination coverage. However, not being able to ensure high 3-dose completion rates should not preclude the initiation of hepatitis B vaccination in STD clinics. Among healthy young adults, protective levels of antibody develop in 30%--55% following a single dose of hepatitis B vaccine and in 75% after 2 doses (5--7). Although long-term (i.e., >10 years) protection cannot be ensured with incomplete vaccination, most persons responding to the first dose are expected to have protection for at least 5 years, which parallels their expected loss of antibody (8). Vaccination completion rates should be monitored, and efforts to increase series completion, especially among those at the highest risk (e.g., MSM and IDUs), should be strongly considered. Reimbursement remains a major barrier to hepatitis B vaccination of persons at increased risk for infection. Sites (e.g., STD clinics) that serve adolescents aged <19 years can obtain and offer vaccination through reimbursement under the Vaccines for Children (VFC) program (http://www.cdc.gov/nip/vfc). In the San Diego VHPP, the majority of sites were enrolled with the state vaccination program as VFC providers. However, vaccination of adults was supported only through funding provided by the project. Private- and public-sector health insurance plans rarely cover hepatitis B vaccination for adults. Although some states and local jurisdictions provide hepatitis B vaccine in STD clinics (9), drug-treatment clinics, and prison health programs, many adults with high-risk medical or behavioral conditions have limited access to recommended vaccinations. Providing additional funding to purchase vaccine for uninsured and underinsured adult populations (10) would overcome a major barrier to vaccinating persons at high risk. The findings in this report are subject to at least three limitations. First, sites for integration of hepatitis B vaccination services were selected on the basis of convenience and might not be representative of all sites. Second, the eligibility criteria used in the STD clinic (i.e., no self-report of previous hepatitis B vaccination or disease) also was used to estimate the percent eligible in all other sites, including sites (e.g., community clinics) that might serve persons for whom hepatitis B vaccination is not specifically recommended. Clinicians at these sites might not have encouraged vaccination for adults without specific risk factors; however, because written risk assessments were not completed for most clients in these settings, the actual percentage of high-risk clients who were offered and received hepatitis B vaccination cannot be determined. Finally, completion rates might be underestimated because persons receiving a first dose of hepatitis B vaccine might not have been followed long enough to track subsequent doses. The findings in this report suggest that a sustained vaccination program, when combined with a short counseling session, might achieve high levels of vaccine acceptance. Even when vaccination cost is not a barrier, achieving high rates of vaccination coverage requires that program managers set vaccination-coverage goals, train staff, review the vaccination status of all clients routinely, and use appropriate health-education materials and counseling services. References
*Sites serving primarily persons with a high risk for HBV infection included clinics providing treatment for sexually transmitted diseases, centers providing services for men having sex with men, the Job Corps program for disadvantaged youth, clinics providing methadone treatment for injection-drug users, drug-offender rehabilitation programs, and correctional institutions. Sites serving primarily persons with a lower risk for HBV infection included clinics providing family planning services, teen services, university/college health care, and community primary care.
|
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services. |
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 7/18/2002
|
|
|||||
|
HOME |
ABOUT MMWR |
MMWR SEARCH |
DOWNLOADS |
RSS
|
CONTACT
|
|||||
|
|
|||||
|
This page last reviewed 7/18/2002