 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Pertussis Outbreak -- Vermont, 1996Pertussis is increasingly recognized as a disease that affects older children and adults, including fully vaccinated persons (1). This report describes a statewide outbreak of pertussis in Vermont (1995 population: 584,771) in 1996 in a highly vaccinated population, affecting primarily school-aged children and adults, and underscores the need to include pertussis in the differential diagnosis of cough illness in persons of all ages. In Vermont, a clinical case of pertussis is defined as a cough illness lasting greater than or equal to 14 days and at least one of the following symptoms: paroxysmal cough, whoop, or post-tussive vomiting. A confirmed case of pertussis requires a positive laboratory finding either by culture or polymerase chain reaction (PCR), or the patient must meet the clinical case definition for pertussis and have had direct contact with a person with laboratory-confirmed pertussis. During January-June 1996, a total of 10 cases of pertussis were confirmed in Vermont, including five culture-confirmed cases (Figure_1). During July 1996, three additional culture-confirmed cases were reported, all in infants aged less than 4 months. None of the three infants attended day care. On July 30, 1996, a pertussis alert was mailed to all primary-care and emergency department physicians in Vermont, advising them of these cases and requesting that pertussis be considered in the differential diagnosis of patients of all ages with persistent cough illness. During 1996, a total of 280 cases (incidence rate: 47.6 per 100,000 population) were identified throughout the state, including 165 laboratory-confirmed cases (160 by positive culture result and five by PCR). Ages of case-patients ranged from 27 days to 87 years: 12 (4%) were aged less than 1 year; 32 (11%), aged 1-4 years; 42 (15%), aged 5-9 years; 129 (46%), aged 10-19 years; and 65 (23%), aged greater than or equal to 20 years. Children aged 10-14 years accounted for 36% of all cases and for the highest incidence rate (235 per 100,000 population) (Figure_2). Pertussis cases occurred in children and/or adults in 69 schools, (range: 1-19 cases per facility). Among 171 cases identified in school-aged children (i.e., aged 5-19 years), most (64%) were culture-confirmed. Of the 65 case-patients aged greater than or equal to 20 years, 46 (71%) occurred in persons reporting contact with children who had confirmed pertussis or cough illness, including parents (21), neighbors or relatives (12), teachers (six), child-care providers (four), and school bus drivers (three). Symptoms of case-patients included paroxysmal coughing (93%), post-tussive vomiting (54%), and whoops (39%). The median duration of cough was reported as 33 days. Twelve (4%) case-patients were hospitalized, and six (2%) had radiologically confirmed pneumonia. Among 19 case-patients aged 7-47 months who were eligible to have received three or more doses of pertussis vaccine, five (26%) had received less than 3 doses. Of the 155 (99%) case-patients aged 7-18 years whose vaccination status was known, 106 (68%) had received four or more doses of pertussis-containing vaccine. All case-patients reportedly had received pertussis vaccine in the form of diphtheria and tetanus toxoids and whole-cell pertussis vaccine (DTP); none had received any doses of diphtheria and tetanus toxoids and acellular pertussis vaccine (DTaP). VDH mailed alerts to all primary-care and emergency-department physicians on July 30, October 30, and December 10 to update them on the epidemiology of the outbreak. Separate mailings were sent to school nurses, school principals, home-schooling parents, and child-care providers. When a case was identified in a school, letters were sent to parents of schoolchildren to inform them of the illness, describe symptoms of pertussis, and encourage parents to have symptomatic children evaluated by a physician. Persons having had direct contact with respiratory secretions of case-patients were identified and referred for prophylaxis. When two cases were reported within the same elementary school classroom, classmates were referred for prophylaxis with antibiotics. Parents and students were asked about special small group settings, such as sports teams or school clubs, and close contacts from these groups were referred for prophylaxis with antibiotics. The number of reported pertussis cases decreased steadily in 1997. During January-June 1997, a total of 172 confirmed cases were reported, representing a 36% decrease from the last 6 months of 1996. Reported by: S Schoenfeld, MSPH, JK Carney, MD, E Hansen, MSN, R Cameron, MJ Celotti, MS, Vermont Dept of Health. Childhood Vaccine Preventable Diseases Br, Epidemiology and Surveillance Div, National Immunization Program, CDC. Editorial NoteEditorial Note: In 1996, the incidence of pertussis in Vermont (47.6 per 100,000) was higher than any other state (national incidence: 2.9 per 100,000). Aggressive case finding and testing helped document and control this outbreak. The high incidence of pertussis in school-aged children was identified based on a strict case definition and was consistent with previous reports of outbreaks in this age group (2). In 1996, school-aged children accounted for 61% of all reported cases in Vermont, compared with 37% of all cases in the United States (CDC, unpublished data, 1996). Approximately half of the school-aged children with pertussis were fully vaccinated. Waning immunity following whole-cell pertussis vaccination accounts for some cases among vaccinated children in this age group (3). Although factors associated with the high incidence in children aged 10-14 years and lower rates in persons aged greater than or equal to 15 years have not been determined, possible explanations include detection bias or a low incidence of disease among older adolescents because of immunity gained during previously undetected pertussis infection. The lower attack rate among children aged less than 10 years suggests a substantial degree of protection from vaccination, despite the intensity of this outbreak. Vaccination rates in Vermont are among the highest in the United States; in 1996, 97% of children aged 19-35 months had received three or more doses of either diphtheria and tetanus toxoids (DT) or DTP (4). School-entry laws in Vermont require a minimum of three doses of a pertussis-containing vaccine, DT or Td (adult formulation of diphtheria and tetanus toxoids). By age 7 years, five doses of pertussis-containing vaccine are recommended for maximum protection. In Vermont, virtually all pediatric vaccines are supplied at no cost by the VDH. Outbreaks of pertussis among school-aged children are difficult to contain, especially because available pertussis-containing vaccines are not approved for use on or after the seventh birthday, and "catch-up" doses cannot be provided for children aged greater than or equal to 7 years who are not fully vaccinated, or to give booster doses to address waning immunity. Although public health measures to curtail outbreaks occurring in school-aged children include the prompt detection and treatment of cases and prophylaxis of their close contacts, these measures may be suboptimal in controlling pertussis outbreaks in settings where repeated exposures occur over an extended period. In addition, physicians may lack clinical experience with pertussis or do not maintain a high index of suspicion for the disease, particularly in vaccinated children and adults. Physicians may be reluctant to prescribe antibiotic prophylaxis for contacts of unconfirmed cases because of concerns about the over use of antibiotics or the accuracy of the diagnosis when culture results are not available. Laboratory confirmation of pertussis cases is subject to multiple constraints. Testing methodologies that provide a more rapid response than culture are either unreliable, costly, or not yet readily available. Culture remains the most common method of confirmation but is considered no more than 50% sensitive (5). Culture is more likely to be positive when the specimen is obtained in the early stages of cough illness; nonetheless, 58% of cases in Vermont were confirmed by culture. Confirmation of cases among vaccinated adolescents and adults was an important adjunct in this investigation and supported the implementation of public health recommendations. Because of the cyclical nature of pertussis outbreaks, periodic reemergence of pertussis epidemics can be anticipated (6). Health professionals in the public and private sectors should assist communities in achieving the highest possible vaccination levels. Even among highly vaccinated populations, waning immunity leads to a substantial population of susceptible older children and adults. During pertussis outbreaks, infection in these age groups may result in exposure of unprotected infants at risk for the most severe consequences of infection (7). Physicians should include pertussis in the differential diagnosis of coughing illness in persons of all ages, use diagnostic testing appropriately, and report suspected cases promptly to the health department. When pertussis is confirmed in the community, health departments should alert providers and the public. Until approved booster vaccination for pertussis is available to protect older children and adults, the prompt diagnosis and treatment of cases and prophylaxis of contacts are the only options for limiting transmission. References
Figure_1 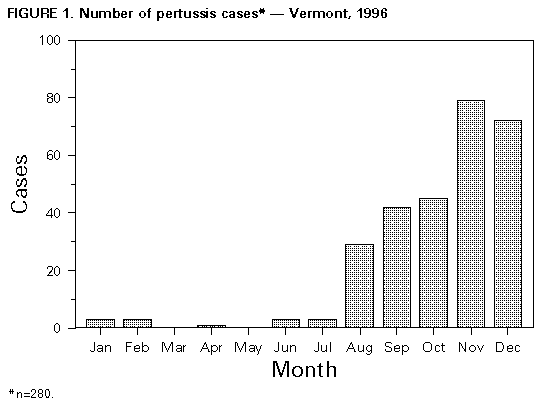 Return to top. Figure_2 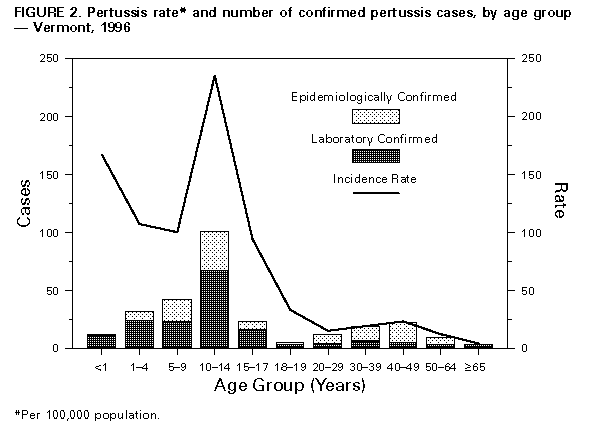 Return to top. Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 09/19/98 |
|||||||||
This page last reviewed 5/2/01
|
{kind=link}
{kind=link}