 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
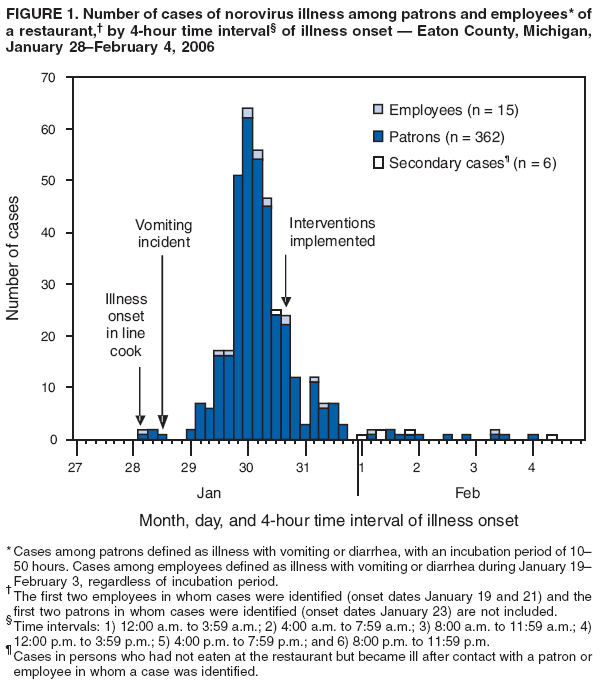
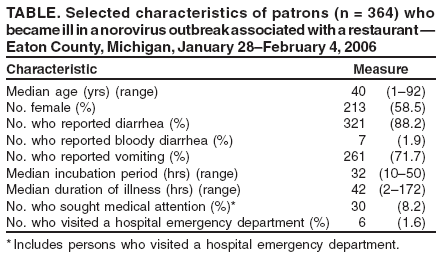
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Norovirus Outbreak Associated with Ill Food-Service Workers --- Michigan, January--February 2006On January 30, 2006, the Barry-Eaton District Health Department (BEDHD) in Michigan was notified of gastrointestinal illness in several members of two dining parties after a meal at an Eaton County restaurant on January 28. An investigation was initiated by BEDHD to identify the source and agent of infection and to determine the scope of illness among patrons and employees of this national chain restaurant. Norovirus genogroup I (GI) was detected in stool specimens submitted by multiple patrons and employees. The investigation revealed that several food-service workers had been ill during January 19--February 3, 2006, and that a line cook had vomited in the restaurant on January 28, possibly increasing environmental contamination and transmission of virus. This report summarizes the findings of the outbreak investigation, which determined that at least 364 restaurant patrons had become ill. The findings underscore the need for 1) ongoing education of food-service workers regarding prevention of norovirus contamination and transmission; 2) enforcement of policies regarding ill and recently ill food-service workers; and 3) environmental decontamination with effective disinfectants to eliminate the presence of norovirus. After learning of the outbreak on January 30, BEDHD launched an epidemiologic and environmental assessment. The restaurant was open for dinner on weekdays and lunch and dinner on weekends and served up to 800 persons daily with a staff of 32--50 employees. Initial investigation indicated that the index case was in an employee who worked as a server at the restaurant and became ill with symptoms of vomiting on or around January 19. Work records indicated that this employee did not work while ill. A second employee (a sibling to the server) became ill with abdominal cramps, diarrhea, and vomiting on January 21 and worked on the first and second days of illness; this person's duties included bartending and administrative work. Seven patrons reported that they had eaten at the restaurant during January 21--27. On January 28, a line cook (line cook A) vomited at home (at approximately 6:00 a.m.) before reporting to work at 11:00 a.m., then vomited again into a waste bin beside the frontline workstation at approximately 2:00 p.m. while preparing antipasti platters, pizzas, and salads. After vomiting, line cook A remained on site (but off the cooking line) and left work at 4:15 p.m. This person also reported to work on January 29 from 11:00 a.m. to 4:30 p.m. while still experiencing loose stools. BEDHD began case finding by obtaining names of patrons from credit card receipts, records of delivery and catering events, and records of dinner reservations; information on patrons without reservations or those who paid with cash was not available. Using Internet-based telephone directories, BEDHD contacted patrons who dined at or consumed food prepared by the restaurant during January 19--February 3. Many patrons contacted BEDHD as a result of the extensive media coverage. BEDHD staff members administered patron interviews by telephone; the interviews included questions about basic demographics, date and time of the restaurant meal, food history, and illness history. Restaurant employees were interviewed in person or by telephone and additionally asked about their work schedules for this period. BEDHD conducted two studies: 1) a descriptive study to characterize ill persons and 2) an analytic study to determine whether certain foods were associated with illness. Because only a portion of restaurant patrons could be identified or contacted, a case-control methodology was used for the analytic study. For the descriptive study, a case in a patron was defined as illness in a patron who had eaten food prepared at the restaurant during January 19--February 3 and who had become ill with vomiting or diarrhea within 10--50 hours (1) after eating the food. A case in an employee was defined as illness in an employee who was ill with vomiting or diarrhea during January 19--February 3, regardless of the incubation period. To determine whether any changes occurred in rates of illness among patrons based on the time the meal was eaten, attack rates were calculated in 3-hour intervals for January 28 and 29, by dividing the number of cases in patrons who dined during each time interval by the number of meals served for those periods. For the analytic study, a case-patron was defined as a patron who had eaten food prepared at the restaurant during January 28--29 (the 2 days line cook A worked while symptomatic) and subsequently became ill with vomiting or diarrhea 10--50 hours after eating; a control was a patron who had the same exposure but no gastrointestinal illness. Statistical software was used to perform the analysis. Chi-square and Fisher's exact tests were used in the case-control analysis. Stool specimens, obtained from patrons and employees, were tested for norovirus RNA by reverse transcriptase--polymerase chain reaction (RT-PCR) and for bacterial pathogens at the Michigan Department of Community Health (MDCH). All positive RT-PCR specimens were genotyped by sequence analysis. Descriptive StudyA total of 625 persons were interviewed by BEDHD: 584 patrons (113 were well), 32 employees, and nine additional persons who became ill after contact with a patron or employee in whom a case was identified. A total of 364 patrons of the 584 interviewed met the descriptive study case definition; the median age was 40 years (range: 1--92 years), 58.5% were female, 88.2% reported diarrhea, 71.7% reported vomiting, and the median duration of illness was 42 hours (range: 2--172 hours) (Table). Patron onset of illness peaked during 12:00 a.m.--3:59 a.m. on January 30 (Figure 1). The median time from a meal at the restaurant until onset of symptoms was 32 hours. The number of cases was already decreasing on January 30, when BEDHD was notified and interventions were implemented. A total of 281 patrons in whom cases were identified had dined on January 28, resulting in an attack rate of 33.7%; on January 29, the attack rate was 13.5% (64 cases divided by 475 meals). Analysis of patron illness based on date and time that the meal was eaten demonstrated that norovirus transmission was occurring in the restaurant before the vomiting incident on January 28 (Figure 2). The attack rate was highest for patrons who ate during 5:00 p.m.--7:59 p.m. on January 28. Transmission continued through the next day. Of the 32 employees interviewed, cases were identified in 17 (53.1%). Seven (41.2%) of these 17 employees had worked while ill during January 21--30. Twelve employees (other than line cook A) worked on January 28 and subsequently became ill. Five (62.5%) of the eight line cooks who worked on January 28 became ill on or after January 28, compared with six (28.6%) of 21 servers. Analytic StudyIn the case-control study of patrons from the period January 28--29, a total of 45 were classified as case-patrons, and 91 were classified as controls. Two foods were found to have a statistically significant association with illness: the antipasti platter (odds ratio [OR] = 2.96; 95% confidence interval [CI] = 1.08--8.14) and garlic mashed potatoes (OR = 4.05; CI = 1.37--11.99). Eighteen patrons (10 who were ill and eight who were well) reported eating the antipasti platter. Sixteen patrons (10 ill and six well) reported eating the garlic mashed potatoes. Nine persons who had not eaten or worked at the restaurant became ill after contact with either a case-patron or case-employee (i.e., household or work contacts). Eight of these nine persons had symptoms of vomiting or diarrhea with illness onset during January 30--February 7. All 14 stool specimens tested by RT-PCR were positive for norovirus GI. The companion bacterial samples tested negative. Results from the sequence analysis, using the degenerative primer set to produce a 213-bp amplicon of region B of the norovirus genome, demonstrated 100% sequence homology with the genotype GI/4 Chiba. Environmental AssessmentThe BEDHD environmental assessment of the restaurant identified deficiencies with employee hand-washing practices, cleaning and sanitizing of food and nonfood contact surfaces, temperature monitoring and maintenance of potentially hazardous food, and maintenance of hand-sink stations for easy accessibility and proper use. Three interventions were undertaken by the restaurant beginning January 30: 1) all food prepared during January 27--30 was discarded; 2) all ill employees were excluded from working for at least 72 hours after their symptoms had subsided; and 3) the facility was cleaned extensively. On February 3, BEDHD received reports of illness in three patrons who had dined at the restaurant on February 1, raising concern that residual contamination remained. Also on February 3, while reviewing the restaurant's clean-up procedures after the vomiting incident, BEDHD sanitarians discovered the restaurant had used a quaternary ammonium-based sanitizer that was ineffective against norovirus. BEDHD instructed the restaurant to disinfect according to MDCH and Michigan Department of Agriculture guidelines for environmental cleaning and disinfection of norovirus (2). The restaurant completed the disinfection with bleach solution before opening at 4:00 p.m. on February 3. Reported by: SR Bohm, MS, BM Brennan, MSPH, Michigan Dept of Community Health; R Schirmer, MD, G Cabose, Barry-Eaton District Health Dept, Charlotte, Michigan. Editorial Note:Norovirus can be transmitted person-to-person (via the fecal-oral route) and spread through contaminated airborne droplets, food, water, environmental surfaces, and fomites (3). In the outbreak described in this report, at least 364 restaurant patrons became ill with gastroenteritis after dining at a restaurant where employees had reported to work while ill. In a norovirus outbreak, a vomiting incident is a major risk factor for norovirus illness and can double the attack rate (4). In this outbreak, vomiting by a line cook at the work station might have contributed to transmission. Because of the open physical layout of the restaurant, no barrier impeded airborne spread of the virus from the kitchen to the main dining area. Attack rates increased after this incident, and among employees who worked on January 28, a higher percentage of line cooks became ill compared with servers. In addition, other environmental contamination probably contributed to transmission. Low-level transmission was occurring in the week before January 28; seven patrons who dined at the restaurant during January 21--27 met the case definition. During January 21--February 3, exposure to virus likely occurred by contact with contaminated surfaces and objects. Foodborne transmission also might have contributed to the outbreak. The antipasti platter (a combination of calamari, bruschetta, and mozzarella cheese sticks with marinara sauce) was one of many dishes that line cook A prepared but the only item among those line cook A prepared that had a statistically significant association with illness. The other food that was linked with illness was the garlic mashed potatoes. However, only a small proportion of patrons ate either of these items. Feline calicivirus, a proxy virus used for norovirus research, can persist in the environment for 21--28 days and is resistant to inactivation by certain cleaning agents (e.g., quaternary ammonium-based sanitizers) (5). In this outbreak, the restaurant's use of cleaning cloths soaked with a quaternary ammonium-based cleaning product likely was ineffective in disinfecting the restaurant (6).* In 2006, MDCH received 144 reports of suspected or confirmed norovirus outbreaks throughout Michigan, compared with 34 in 2005 (MDCH, unpublished data, 2007). Norovirus genogroup II (GII) was identified in 97% of the 89 confirmed outbreaks in the state during 2006; GI was identified in the remaining 3% of the outbreaks. During 2000--2004, the predominant genogroup in calicivirus outbreaks in the United States was GII (79%), followed by GI (19%) and sapovirus (2%) (7). No other GI/4 outbreaks were detected in Michigan in 2006. In this outbreak, the detection of one norovirus genogroup (GI/4) in all stool specimens, including that of line cook A, suggests a single source of infection. Approximately 50% of all norovirus outbreaks are linked to ill food-service workers (8). The Michigan Food Law of 2000,† which regulates Michigan food establishments, requires that food-establishment operators notify regulators when employees have infections with Salmonella, Shigella, Escherichia coli O157:H7 or hepatitis A. Food-service employees in Michigan also are obliged under the food law to inform their supervisors when they have symptoms of illness, such as diarrhea and vomiting. In October 2007, Michigan adopted several amendments to the Michigan Food Law of 2000, including the 2005 Food and Drug Administration Food Code.§ The 2005 Food Code includes norovirus as one of several highly pathogenic organisms that can be easily spread by ill food handlers and provides disease-specific conditions for work exclusion, restriction, and reinstatement. After the outbreak described in this report, BEDHD issued four recommendations (based on previously published guidelines [9]) for infection control and environmental decontamination after any vomiting incident in a food-service establishment. First, any exposed food or single-service articles (e.g., drinking straws, takeout containers, and paper napkins) should be discarded, and all surface areas within at least a 25-foot radius of the vomiting site should be disinfected with a bleach solution (2). Second, ill employees should be excluded from work for at least 72 hours after symptoms subside, and employees returning after a gastrointestinal illness should be restricted from handling kitchenware or ready-to-eat food for an additional 72 hours. Third, because thorough disinfection might be necessary, partial or complete closure of the food establishment should be considered after a vomiting incident. Finally, restrooms used during or after a vomiting incident should be closed immediately until they are disinfected properly with bleach solution. Acknowledgments This report is based, in part, on contributions by the Barry-Eaton District Health Dept; E Belk, P Clark, V Leykam, L Mosher, J Massey, S Bidol, J Collins, S Johnson, C Miller, MG Stobierski, M Wilkins, A Mattson, Michigan Dept of Community Health; and L Hainstock, Michigan Dept of Agriculture. References
* The Environmental Protection Agency has approved the claims of effectiveness against norovirus of several antimicrobial disinfectants. Some of these products include quaternary ammonia-based disinfectants but are in combination with alcohols. These claims of effectiveness are based on in vitro studies that typically use a proxy virus (e.g., feline calicivirus); field effectiveness in the context of outbreaks has not been evaluated. A list of these products is available at http://www.epa.gov/oppad001/list_g_norovirus.pdf. † Available at http://www.michigan.gov/mda/1,1607,7-125-1568_2387_2435---,00.html. § Available at http://www.cfsan.fda.gov/~dms/fc05-toc.html. Figure 1
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Date last reviewed: 11/20/2007 |
|||||||||
|