
Case #135 - July, 2004
A 51-year-old man was brought to the emergency room after a friend noticed he was minimally responsive. The friend explained that the patient had been suffering from upper respiratory symptoms and mild fever for about three weeks, and a progressive cough for about one week. A chest X-ray revealed a large, left pleural effusion and a right mediastinal shift. A chest tube released two liters of pressurized, odoriferous purulent fluid. The pleural fluid was sent to the laboratory for complete microbiological work-up. Figures A–D show what was observed on slide preparations stained with Wright-Giemsa. What is your diagnosis? Based on what criteria?
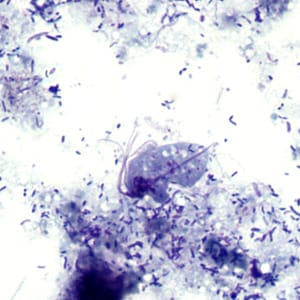
Figure A
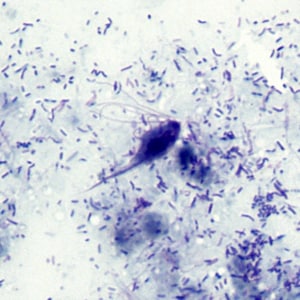
Figure B
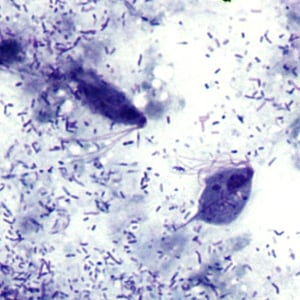
Figure C
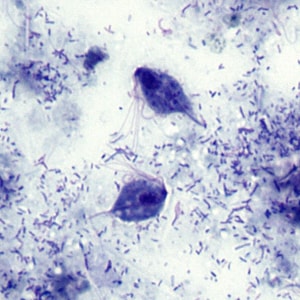
Figure D
This case and images were kindly provided by Alameda County Medical Center, Oakland, CA.
Images presented in the monthly case studies are from specimens submitted for diagnosis or archiving. On rare occasions, clinical histories given may be partly fictitious.
DPDx is an educational resource designed for health professionals and laboratory scientists. For an overview including prevention, control, and treatment visit www.cdc.gov/parasites/.