 ShareCompartir
ShareCompartir

Monthy Case Studies - 2003
Case #120 - November, 2003
A middle-aged man from East Africa, who had immigrated to the United States 20 years ago, had an intermittent fever for two weeks, which progressed to a daily fever with chills. He had also experienced severe weight loss during the previous six months. He had traveled to Southeast Asia while living outside the U.S., and his past medical history revealed he had contracted malaria twice. It was also discovered that he was positive for HIV by antibody testing. A CT scan revealed that he had an enlarged spleen and liver. A bone marrow aspirate was obtained and part of it was stained with hematoxylin and eosin (H & E) and the rest used to inoculate a culture. Figures A and B show what was seen in the stained aspirate. Figures C and D show what was seen on a Giemsa stained smear from the culture 10 days postinoculation. What is your diagnosis? Based on what criteria?
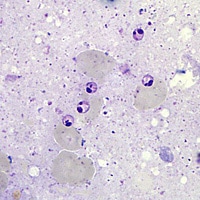
Figure A
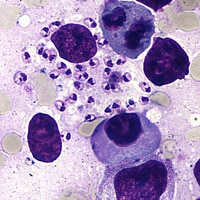
Figure B

Figure C

Figure D
Acknowledgement: This case kindly provided Dr. Lisa Mahnke, Washington University School of Medicine, St. Louis, MO.
Answer to Case #120
This was a case of leishmaniasis caused by Leishmania sp. As the specimen used for diagnosis was a bone marrow aspirate, in all probability this was a case of visceral leishmaniasis. However, only techniques such as PCR or isoenzyme analysis can confirm the species of Leishmania causing disease. This particular case was an example of reactivated visceral leishmaniasis (kala-azar) precipitated by a CD4 count decline secondary to the patient acquiring HIV. The species was determined to be L. donovani by isoenzyme analysis at CDC following culture of the organism. Diagnostic features observed included:
- the presence of amastigotes (Figures A and B) in the bone marrow aspirate. One can clearly see a well-defined nucleus and kinetoplast in most of the parasites in the two images. Depending on the specimen, the amastigotes could represent an infection with Leishmania spp. or Trypansoma spp. Genus and species determination should not be based on observation of amastigotes alone.
- the presence of promastigotes (Figures C and D), the flagellated forms, in culture. At this point a distinction between Leishmania spp. and Trypansoma spp. can be made if the laboratorian prepares a Giemsa stained smear and has experience with the morphology of these organisms. However, a final genus and species determination should not be made on visual observation alone.
More on: Leishmaniasis
Images presented in the monthly case studies are from specimens submitted for diagnosis or archiving. On rare occasions, clinical histories given may be partly fictitious.
