Volume
8: No. 2, March 2011
Diane Allensworth, PhD; Theresa C. Lewallen, MEd; Beth Stevenson, MPH; Susan Katz, MPH
Suggested citation for this article: Allensworth D, Lewallen TC, Stevenson B, Katz S. Addressing the needs of the whole child: what public health can do to answer the education sector’s call for a stronger partnership. Prev Chronic Dis 2011;8(2):A44.
http://www.cdc.gov/pcd/issues/2011/mar/10_0014.htm.
Accessed [date].
PEER REVIEWED
Abstract
Although the overall level of child health in the United States remains high, public health professionals know that racial and ethnic disparities in child and adolescent health persist and that lifestyle choices related to chronic disease in adults are often established in childhood and adolescence. And yet, those health needs are not the public health sector’s alone to resolve. We have natural partners among educators.
Improving graduation rates is one of the most cost-effective ways
to reduce health disparities. This article provides strategies for how public
health professionals can answer this call by educators to address the needs
of the whole child.
Back to top
Background
Education and health are interdependent systems that increasingly need to collaborate in helping our nation’s children. The authors of The Learning Compact Redefined: A Call to Action
recommend that local schools work closely with the public health community to
adequately address the conditions that affect learning (1). This call represents
both a challenge and an opportunity for the public health community. Not only do
public health data indicate that education levels and health outcomes are highly
correlated but public health professionals also have pressing needs to reach
students to achieve health outcomes.
Health and education are integrally linked (2). Children who do not complete
high school are likely to become adults who have employment problems, lower health literacy, higher rates of illness, and earlier deaths than those who
graduate from high school (3,4). Evidence suggests that improving high school
graduation rates may be more cost-effective than most medical interventions in
reducing health disparities (3,5). Graduation from high school is associated
with an increase in average lifespan of 6 to 9 years (6). The reasons students
drop out of school are complex (7), and health can be integrally related to many
of these reasons, including barriers to learning such as hunger and poor
nutrition and even fear for safety at school (8). Health problems contribute to
absenteeism and, in turn, absenteeism (9) as well as unintended pregnancy and delinquency (5) are associated with dropping out of school. Other risk factors for dropping out are frequent changes of schools, lack of parent participation in
schooling, and nonproductive use of leisure time, such as watching many hours of television daily (8).
The United States ranks 18th among nations in high school completion rates (10). Every school day, 7,000 students drop out of school, resulting in 1.2 million dropouts annually (3). Although generally the percentage of students in the United States who complete school is close to 70%, the rates for poor Native American, African American, and Hispanic students are substantially lower. In some
urban areas the number of Hispanic and African American male students who graduate is less than 50% (9).
Dropping out of school contributes to future unemployment or underemployment, and dropouts are more likely to commit crime or rely on government assistance for health care, housing, and food. Dropouts are less likely to raise healthy, well-educated children (3). A combination of underlying health, family, community, and education issues must be addressed to prevent this cycle. No one sector can address the complexity of the interdependent needs of children.
Previous studies have found that when the public health and
education sectors work together and collaborate with community agencies,
students’ academic achievement and health improve (11-14).
Back to top
Educators Request Public Health Involvement
Educators recognize that a focus on academic achievement as a means to ensure graduation requires a concomitant focus on the areas that support learning — including
safety and physical, mental, and social health. Research indicates that students are more successful in school and in life when they experience a broad, challenging, and engaging curriculum; when they feel connected to their school and surrounding community; when their physical and emotional health is supported; and
when schools offer safe and nurturing environments (15-22). By providing these conditions, schools and the community address the cognitive, physical, social, and emotional well-being of the whole child and support children’s growth and development into knowledgeable, healthy, and productive adults.
To address these conditions for supporting children, in 2006, ASCD, a professional educational association (formerly The Association for Supervision and Curriculum Development), commissioned an interdisciplinary panel that included public health leaders to develop The Learning Compact Redefined: A Call to Action
(1). This report challenges schools and communities to work together in new ways
to develop “successful learners who are knowledgeable, emotionally and
physically healthy, civically active, engaged, prepared for economic
self-sufficiency, and ready for the world beyond formal schooling (23).” The Learning Compact Redefined: A Call to Action (1) is designed around
the following 5 elements for the nation’s students:
- Each student enters school healthy and learns about and practices a healthy lifestyle.
- Each student learns in an intellectually challenging environment that is physically and emotionally safe for students and adults.
- Each student is actively engaged in learning and is connected to the school and broader community.
- Each student has access to personalized learning and to qualified and caring adults.
- Each graduate is prepared for success in college or further study and for employment in a global environment.
These 5 elements provide a framework for how health and education can begin to work together to achieve mutual goals.
Back to top
A Public Health Rationale for an Expanded Partnership
Schools are one of the most efficient systems for reaching children and youth to provide health services and programs, and approximately 95% of all US children and youth attend school (24). Establishing healthy behaviors during childhood is easier and more effective than trying to change unhealthy behaviors during adulthood and affords the population more years of healthy life. Schools play a critical role because of these factors:
- Each school day is an opportunity for the nation’s 55 million students to learn about health and practice the skills that promote healthy behaviors.
- The nation’s 125,000 schools have the potential to provide opportunities for students to practice healthy behaviors such as eating healthy foods and participating in physical activity (25).
To illustrate the relationship between health and education from the perspective of The Learning Compact Redefined: A Call to Action, we developed a model that portrays some of the factors that can affect the health and education of children and youth (Figure 1). The Learning Compact Redefined: A Call to Action recognizes that health and education are interdependent and can result in better health and education outcomes, increased graduation rates, and ultimately, healthier adults
who will have healthier children. The model describes an interdependent process where increases in which high school graduation rates are linked to improved health outcomes.
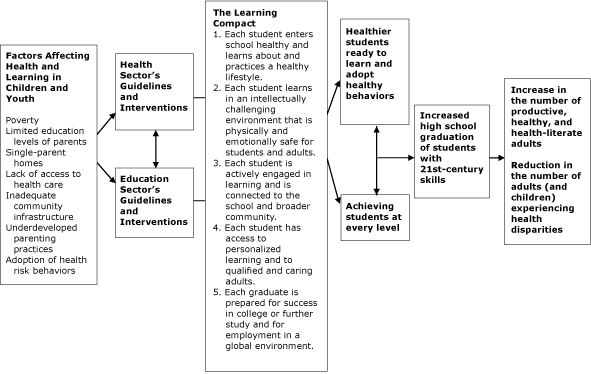
Figure. The Learning Compact for Children can
link the health sector and the education sector in a collaborative effort
that addresses the social determinants of health and promotes better
learning and health outcomes for children and the adults that they will
become. [A text description of this figure is
also available.]
Back to top
Strengthening the Partnerships Between Health
and Education
Although school districts and health departments have historically worked together and best practices from coordinated school health program examples encourage schools to involve community agencies (26), it is not standard in many communities for the public health department to provide services to schools. A 2008 survey of local health department jurisdictions found that only 36% of these jurisdictions conducted school health activities (27).
Despite challenges to collaborative work between public health and education, both sectors are adept at partnerships, and successes are emerging with demonstrated partnership activities. The interdisciplinary panel that developed The Learning Compact has recommended that public health and education sectors in every community discuss steps to ensure that the conditions for learning are met. For the public health sector, this conversation must begin with the understanding that
today’s educational practice and policies focus overwhelmingly on academic achievement. The National Association of State Boards of Education’s resource How Schools Work and How to Work with Schools provides questions that public health professionals can ask to begin the conversation using education-focused questions (28).
- What do we want from schools?
- What can we offer schools?
- Whom should I contact within the education system?
- How is our agenda related to what’s important to education leaders?
Similarly, educators should ask what they need from public health, what education can offer, and how health and education agendas can work together to reach
mutual health and education outcomes.
We present strategies that public health agencies could use to support education and
to address the 5 elements of The Learning Compact
(Table 1). Strategies to be implemented would be based on conversations between the 2 sectors.
Since The Learning Compact was published, ASCD has supported partnership initiatives between education and public health that are based on an understanding of the interdependent nature of education and health outcomes and driven by the 5 elements of the learning compact. ASCD conducted a 3-year evaluation of its 11 Healthy School Communities pilot sites, which looked at how well those sites addressed the principles of The Learning Compact.
Student outcomes improved at sites where the school and
public health agencies worked together to meet their mutual goals. For example, in Des Moines, New Mexico, and
in Indianapolis, Indiana, school-based health care and wellness centers provide services to
students, their families, and community members. Student attendance and discipline referrals — factors that correlate with graduation rates — have improved since
the establishment the health centers. In Hills, Iowa, where access to fresh produce is limited, the public health department provides health education as
well as fruits and vegetables in a low-income elementary school. At the same time, the school implemented a research-based approach to
improving school climate. The school reports fewer discipline problems and improvement in reading and math, which is attributed to students’ better nutrition and changes to the school climate. Other public
health relationships of the Healthy School Communities pilot sites include the school district and public health agency sharing the cost of providing nurses in the schools for health screenings and referrals and coordinating the district’s implementation of an evidence-based health program (29). The key factor in each of these partnerships is the role that the public health staff played in the school improvement process — working with the school improvement team to make systemic,
sustainable change in the school environment through policy and practice that align with the schools’ mission, vision, and goals (RF Valois,
unpublished report, 2009).
Back to top
Summary
The Learning Compact Redefined: A Call to Action recommends that local schools work closely with the public health community to address conditions that affect learning. Not only do public health data indicate that education levels and health outcomes are highly correlated but
health officials also have pressing needs to address the current health needs of children as well as to promote behaviors that will affect health throughout their lifespan. Education and health are interdependent systems that urgently need to
collaborate in helping our nation’s children. Together, public health and education can reduce absenteeism, improve achievement, and increase graduation rates. In turn, improved graduation rates will help reduce health disparities and increase the quality and years of healthy life — 2 major goals of the public health sector and the nation. Such outcomes can help curtail the intergenerational cycle of poverty that is the underlying factor for many public health problems. The public
health sector has a vital role to play in responding to the call from educators. We can no longer afford to consider the work of
public health and education as separate paths to our respective outcomes. The 5 elements of the learning compact provide a framework for education and health to work more closely together to address the health and education needs of all students.
Back to top
Author Information
Corresponding Author: Diane Allensworth, PhD, Centers for Disease Control and Prevention 4770 Buford Hwy, Mailstop E-73, Atlanta, GA 30333. Telephone: 770-488-5353. E-mail:
dda6@cdc.gov.
Author Affiliations: Theresa C. Lewallen, ASCD, Alexandria, Virginia; Beth
Stevenson, Susan Katz, Centers for Disease Control and Prevention, Atlanta,
Georgia.
Back to top
References
- The learning compact redefined: a call to action. A report of the
Commission on the Whole Child. ASCD; 2007. http://www.ascd.org/ASCD/pdf/Whole%20Child/WCC%20Learning%20Compact.pdf. Accessed April 11, 2010.
- Murray NG, Low BJ, Hollis C, Cross AW, Davis SM.
Coordinated school health programs and academic achievement: a systematic review of the literature. J Sch Health 2007;77(9):589-600.
- Alliance for Excellent Education. The high cost of high school dropouts: what the nation pays for inadequate high schools; 2008. http://www.all4ed.org/publications/HighCost.pdf. Accessed May 5, 2008.
- Pappas G, Queen S, Hadden W, Fisher G.
The increasing disparity in mortality between socioeconomic groups in the United States, 1960 and 1986. N Engl J Med 1993;329(2):103-9.
- Freudenberg N, Ruglis J. Reframing school dropout as a public health issue. Prev Chronic Dis 2007;4(4).
http://www.cdc.gov/pcd/issues/2007/oct/07_0063.htm.
- Wong MD, Shapiro MF, Boscardin WJ, Ettner SL.
Contribution of major diseases to disparities in mortality. N Engl J Med 2002;347(20):1585-92.
- Rumberger R. Why students drop out of school. In: Orfied G, editor. Dropouts in America: confronting the graduation rate crisis. Cambridge (MA): Harvard Education Press; 2004. p. 131-55.
- Barton PE, Coley R. Parsing the achievement gap II. Princeton (NJ): Educational Testing Services; 2009. http://www.ets.org/Media/Research/pdf/PICPARSINGII.pdf. Accessed October 18, 2010.
- Allensworth E, Eston JQ. What matters for staying on track and graduating in Chicago public high schools. Chicago (IL): Consortium on Chicago School Research at the University of Chicago, Research Report; 2007.
- Hodgkinson HB. The whole child in a fractured world. Alexandria (VA): Association for Supervision and Curriculum Development; 2006.
- Vinciullo FM, Bradley BJ.
A correlational study of the relationship between a coordinated school health program and school achievement: a case for school health. J Sch Nurs 2009;25(6):453-65.
- Getting results: developing safe and healthy kids. California
Department of Education; 2008. http://www.cde.ca.gov/ls/he/at/gettingresults.asp. Accessed February 14, 2009.
- Making the connection: health and student achievement. Society of State Directors of Health, Physical Education, and Recreation (SSDHPER), Association of State and Territorial Health Officials (ASTHO); 2002.
http://www.thesociety.org/pdf/makingtheconnection.ppt. Accessed November 8, 2010.
- Blank MJ, Shah BP. Educators and community sharing responsibility for student learning.
Successful Practices Network. Infobrief; 2004.
http://www.ascd.org/publications/newsletters/infobrief/jan04/num36/toc.aspx.
Accessed November 29, 2010.
- Barton PE. Parsing the achievement gap. Princeton (NJ): Educational Testing Service; 2003.
- Getting results: update 5 — Student health, supportive schools, and academic success. California Department of Education. Sacramento (CA): CDE
Press; 2005.
- Health Behaviors in School-Age Children (HBSC) 2005/2006 Survey: School Report (NA).
Department of Health and Human Services, National Institutes of Health. Washington (DC): US Government Printing Office; 2008.
- Laitsch D, Lewallen T, McCloskey M. A framework for education in the 21st century. Infobrief 2005;40:1-8.
http://www.ascd.org/publications/newsletters/infobrief/feb05/num40/toc.aspx.
Accessed November 29, 2010.
- Every child learning: safe and supportive schools. Learning First Alliance. Alexandria (VA): Association for Supervision and Curriculum Development; 2001.
- Rothstein R. Class and schools: using social, economic, and educational reform to close the black-white achievement gap. Washington (DC): Economic Policy Institute; 2004.
- The condition of education 2005. US Department of Education, National Center for Education Statistics (NCES 2005–094). Washington (DC): US Government Printing Office; 2005.
-
Wingspread
Declaration on School Connections. J Sch Health 2004;74(7):233-4.
- The Community Conversations Project: a guide for informal discussion groups. ASCD; 2007. http://www.ascd.org/ASCD/pdf/Whole%20Child/whole%20child%20community%20conversations%20no%20date.pdf. Accessed April 11, 2010.
- Fisher C, Hunt P, Kann L, Kolbe L, Patterson B, Wechsler H. Building a healthier future through school health programs.
Centers for Disease Control and Prevention; 2004.
http://www.cdc.gov/HealthyYouth/publications/pdf/PP-Ch9.pdf. Accessed April 11, 2009.
- Coordinated School Health Programs (CSHP). Healthy Youth 2008. http://www.cdc.gov/healthyYouth/about/healthyyouth.htm. Accessed March 2, 2009.
- Allensworth DD. Promoting the diffusion of coordinated school health programs. Presentation, DASH Funded Partners Meeting. Atlanta, Georgia; April 10, 2007.
- National Association of City and County Health Officials. 2008 National
profile of local health departments, 2009. http://www.naccho.org/topics/infrastructure/profile/resources/ 2008reports/upload/NACCHO_2008_ProfileReport_post-to-website-2.pdf. Accessed April 10, 2010.
- Bodgen JE. National Association of State Boards of Education (NASBE).
How schools work and how to work with
schools: a primer for professionals who serve children and
youth. Alexandria (VA): National Association of State Boards of
Education; 2003.
- Community Access To Child Health (CATCH).
http://www.aap.org/catch/. Accessed April 3, 2010.
Back to top
