Volume
8: No. 4, July 2011
Gwen Hosey, MS, ARNP, CDE; Henry Ichiho, MD, MPH; Dawn Satterfield, PhD, RN; Irene Dankwa-Mullan, MD, MPH; Stevenson Kuartei, MD; Kyu Rhee, MD, MPP; Tayna Belyeu-Camacho; Ione deBrum; Yorah Demei; Kipier Lippwe; Patrick Solidum Luces; Faiese Roby, MD
Suggested citation for this article: Hosey G, Ichiho H, Satterfield D, Dankwa-Mullan I, Kuartei S, Rhee K, et al. Chronic disease surveillance systems within the US associated Pacific Island jurisdictions. Prev Chronic Dis 2011;8(4):A86.
http://www.cdc.gov/pcd/issues/2011/jul/10_0148.htm. Accessed [date].
PEER REVIEWED
Abstract
In recent years, illness and death due to chronic disease in the US Associated Pacific Islands (USAPI) jurisdictions have dramatically increased. Effective chronic disease surveillance can help monitor disease trends, evaluate public policy, prioritize resource allocation, and guide program planning, evaluation, and research.
Although chronic disease
surveillance is being conducted in the USAPI, no recently published
capacity assessments for chronic disease surveillance are available. The objective of this study was to
assess the quality of existing USAPI chronic disease data sources and identify jurisdictional capacity for chronic disease surveillance. The assessment included a chronic disease data source inventory, literature review, and review of surveillance documentation available from the web or through individual jurisdictions. We used the World Health Organization’s Health Metric Network
Framework to assess data source quality and to identify jurisdictional capacity. Results showed that USAPI data sources
are generally aligned with widely accepted chronic disease surveillance indicators and use standardized data collection methodology to measure chronic disease behavioral risks, preventive practices, illness, and death. However, all jurisdictions need to strengthen chronic disease surveillance through continued assessment and expanded support for valid and reliable data collection, analysis and reporting, dissemination, and integration among population-based and institution-based data
sources. For sustained improvement, we recommend investment and technical assistance in support of a chronic disease surveillance system that integrates population-based and institution-based data sources. An integrated strategy that bridges and links USAPI data sources can support evidence-based policy and population health interventions.
Back to top
Introduction
Although chronic disease has long concerned high-income countries, 80% of chronic disease deaths occur in low- to middle-income countries (1). A complex interplay of socioeconomic, demographic, technologic, cultural, environmental, and biological factors explains this epidemiologic transition from communicable disease to noncommunicable disease (NCD) (1,2). The burden of chronic disease is
substantial in the US Associated Pacific Islands (USAPI) jurisdictions (American Samoa, Guam,
Commonwealth of the Northern Mariana Islands [CNMI], Federated States of Micronesia [FSM] [Chuuk, Kosrae, Pohnpei, and Yap], Republic of Palau, and Republic of the Marshall Islands [RMI]). For example, although differences in age-standardizations hinder comparison (3,4), age-standardized cardiovascular disease (CVD) mortality estimates among the USAPI
jurisdictions are generally higher than similar US age-standardized CVD mortality estimates (5,6)
(Table 1).
The USAPI jurisdictions’ population spreads across 104 inhabited islands in more than 3 million square miles of ocean, crossing the International Date Line. Despite the challenges of
geographic isolation, dependence on US and international aid, and lack of health care funding (7), the USAPI
jurisdictions are targeting chronic disease prevention by developing partnerships and approaches that reflect the interface between Pacific cultures and Western science (2,8,9). In addition, a May 2010 Pacific Island
Health Officers Association resolution declaring a state of health emergency due to the epidemic of chronic disease encourages stronger coordination of partnerships across multiple sectors to mobilize policy, investments, and technical resources to reduce the
prevalence and costs of chronic disease within the region (10). Effective chronic disease surveillance systems can support this effort and help the USAPI leadership monitor disease trends, evaluate public policy, prioritize resource allocations, and
guide program planning, evaluation, and research.
Surveillance is defined as the ongoing, systematic collection, analysis, interpretation, and dissemination of data essential for health promotion and disease prevention (11). Chronic disease surveillance data sources supported by the Centers for Disease Control
and Prevention (CDC), World Health Organization (WHO), and USAPI health care systems can be divided into 2 main categories: population-based (ie, household surveys) and institution-based (ie, disease registries) (Figure). The objective of this
study was to assess the quality of existing USAPI chronic disease data sources and identify the capacity for chronic disease surveillance by individual jurisdiction,
following WHO’s Health Metric Network Framework
(HMNF). We also offer recommendations for continued capacity building to strengthen surveillance within the region.
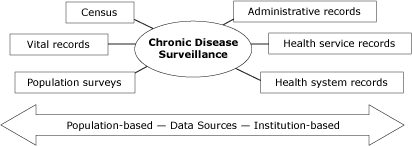
Figure. Potential chronic disease surveillance data
sources. Chronic disease surveillance may include both population-based and
institution-based data sources. Population-based sources include census
data, vital records, and population health surveys. Institution-based
sources include administrative records (eg, tax revenues), health service
records (eg, occupational health), and health system records (eg, disease
registries).
Adapted from Health Metrics Network Framework
(http://www.who.int/healthmetrics/documents/hmn_framework200803.pdf). [A
text description of this figure is also
available.]
Back to top
Methods
After reviewing the literature and documents available on the web or through individual jurisdictions, we established an inventory of data sources for monitoring standard chronic disease indicators (11). Using this list, USAPI chronic disease representatives identified their jurisdictions’ existing data sources, frequency of data collection, and availability of analysis and reporting. For each identified data source, the frequency of data collection, analysis, and reporting was
confirmed by the respective USAPI Ministry of Health or Department of Health administration. CDC verified USAPI participation in the CDC-supported data sources. The US Renal Data System (USRDS) Western Pacific Renal Network verified the Medicare certification dates for jurisdictions participating in the USRDS data network (S. Tanner, oral communication,
April 2011).
We completed a literature search concerning USAPI capacity for chronic disease surveillance through the National Library of Medicine’s and National Institutes of Health’s PubMed
(www.ncbi.nlm.nih.gov/pubmed/) and EBSCO’s
Cumulative Index to Nursing and Allied Health Literature (CINAHL). Publications included meet the following criteria: 1) they assessed chronic disease surveillance capacity for the USAPI region overall or by individual jurisdiction and 2) were published in English within the last 10
years (ie, 1999 through October 2010). We excluded publications that presented only results of USAPI chronic disease-related research (ie, epidemiologic, clinical, and qualitative) or program evaluation without inclusion of an assessment related to chronic disease surveillance in the region overall or by individual jurisdiction. Search terms were “chronic disease,”
“population surveillance,” “disease surveillance,” “American Samoa,”
“Guam/epidemiology,” “Micronesia/epidemiology,” and “Marshall
Islands.” To select the publications, the titles and abstracts were reviewed by
1 author (G.H.) for relevance; those that met the inclusion criteria were selected. Subsequently, the entire text of selected publications was read and publications that did not meet the inclusion criteria were excluded.
We used the WHO HMNF as the foundation for assessing the quality of USAPI chronic disease surveillance data sources and identifying jurisdiction capacity
(Table 2). The HMNF is a global health partnership formed in 2005 that supports assessment and capacity building for health information systems in low- to middle-income countries (12). Two authors
(G.H., H.I.) completed independent assessments for each data source by using supporting documentation retrieved from web-based
archives, literature review, or from surveillance documentation provided by individual jurisdictions. Aggregate scores for each assessment criterion ranged from 3 (highly adequate) to zero (not adequate). We did not score data sources without complete documentation.
Back to top
Results
USAPI data sources are listed by category and data availability by year
(Table 3). A summary
description of each data source follows.
Population-based data sources
The Behavioral Risk Factor Surveillance System (BRFSS) is a standardized survey that includes measures for chronic disease risk factors and conditions, preventive health practices, and access to health care among adults (≥18 y) (www.cdc.gov/brfss/index.htm).
The BRFSS uses a computer-assisted telephone-interviewing system with
participation limited to households with available telephone service.
The WHO STEPwise approach (STEPS) is a standardized population health survey
of adults aged 25 to 64 years that measures chronic disease and associated risk
factors. STEPS involves a 3-step sequential process: 1) a questionnaire
assessing demographic, behavioral, and lifestyle risks; 2) direct
anthropometrical and blood pressure measures; and 3) biochemical assessment of
blood samples (www.who.int/chp/steps/en).
The Youth Risk Behavior Surveillance System (YRBSS) is a standardized national school-based surveillance system that
surveys students in grades 9 through 12 to measure behaviors that contribute to unintentional injuries and violence; tobacco use; alcohol and drug use; unintended pregnancy and sexually transmitted diseases; unhealthy dietary behaviors; and physical inactivity. Participating USAPI jurisdictions conduct the survey every 2 to 4 years (www.cdc.gov/yrbss).
The Youth Tobacco Survey (YTS) is a standardized school-based survey that provides data necessary to support the design, implementation, and evaluation of tobacco
prevention and control programs for students in middle (grades 6-8) and high (grades 9-12) schools. The similar Global Youth Tobacco Survey (GYTS) is a standardized school-based survey (students aged 13-15 years)
designed to build global capacity to monitor youth tobacco use, guide implementation and evaluation of tobacco prevention and control programs,
and compare tobacco use data (www.cdc.gov/tobacco/index.htm). USAPI
jurisdictions generally participate in the YTS every 4 to 5 years. Each USAPI jurisdiction may conduct the YTS or the GYTS.
Institution-based data sources
Disease registries
Cancer. Each jurisdiction collects data on cancer incidence, types, and
sites and extent of cancer at diagnosis. USAPI jurisdictions submit their cancer data to the Pacific Regional Central Cancer Registry, which compiles and reports them to CDC as de-identified cancer information (www.cdc.gov/cancer/npcr).
Renal disease. USRDS is a national data system that collects,
analyzes, and distributes information about end-stage renal disease in the United States (www.usrds.org). Medicare-certified dialysis centers operating in the USAPI contribute data to USRDS. Guam has 4 certified facilities submitting data; American Samoa has 1 certified facility and the CNMI has 2 certified facilities. The USRDS does not include FSM, Palau, or RMI
(because of federal compact agreements).
Health system records
Vital statistics include data on births and deaths (including fetal deaths). For chronic disease surveillance, mortality data are used to track underlying and contributing cause of death and life expectancy. Using standard forms and procedures (ie,
International Classification of Diseases, 10th revision [ICD-10] codes to classify deaths), the National Vital Statistics System (NVSS) within the National Center for Health Statistics estimates mortality rates for American Samoa, CNMI, and Guam (5). Mortality estimates for FSM, Palau, and RMI are
available through WHO (6) or individual jurisdictions.
Hospital discharge data are abstracted records documenting an individual’s hospital stay.
These records include information on patient demographics, diagnosis, treatment, and discharge condition. Individual jurisdictions collect, analyze, and report hospital discharge data.
Literature review data sources
The MEDLINE and CINAHL database search found no published reports regarding assessment of chronic disease surveillance capacity within the USAPI region overall. Haddock
(13) provided a historical perspective of Guam’s communicable disease, vital statistics, cancer, and maternal-child health surveillance. Most published reports were specific to assessment of the USAPI’s capacity for cancer control and prevention (including surveillance), summarized by Tsark and Braun
(14)
and published in Pacific Health Dialog (15).
Assessment of USAPI data sources
The following summarizes data source assessments (Table 4).
Content and scope
In general, the quality of data source content was rated as highly adequate; most jurisdictions reported participation in standardized population-based surveys (ie, BRFSS, YRBSS, GYTS, YTS, or STEPS).
Jurisdictions also reported continual administration of vital
records, disease registries (eg, cancer, USRDS), and other health system records
(eg, hospital discharge). Collectively, these data sources provide most jurisdictions with uniform measures for cancer, CVD, diabetes, tobacco and
alcohol use, physical activity and nutrition, other diseases and risk factors, demographics,
and socioeconomic conditions.
Data collection frequency and the availability of a nationally representative population-based sample vary among jurisdictions. For example, the annual Guam BRFSS uses a representative adult (≥18 y) population sample. In comparison, STEPS uses a sample of representative adults (aged 25-64 y), although individual jurisdictions may adjust the age range of the target population. However, administration of the STEPS survey ranges from every 5 years in Pohnpei
(2002 and 2007) to more than 5 years for American Samoa (2004) and RMI (2002).
Finally, whereas representative data were consistently available for Palau’s YRBS, availability of representative YRBS data from other jurisdictions varied by survey year.
Jurisdictional capacity
Generally, jurisdictional capacity is adequate; jurisdictions rely on US or WHO fiscal, administrative, and technical support for most data sources.
Except for the STEPS survey, most USAPI population-based surveys have weighted
data available by subgroup (ie, age, sex) across survey years. However,
disaggregated analysis by socioeconomic status (ie, income, education, and occupation) is limited to selected measures within the Guam BRFSS. Availability of STEPS disaggregated analysis by socioeconomic status is unavailable for participating jurisdictions.
Dissemination
Dissemination of metadata and microdata files varied across data sources. For example, dissemination of the BRFSS, YRBSS, GYTS, and YTS data analysis and reports was adequate, supported by the availability of reports within 12 months of survey completion and metadata accessible through CDC websites. Microdata are available on request or through web-based data repositories.
In comparison, dissemination of STEPS data analysis and reports
range from present but not adequate (FSM and RMI) (16,17) to adequate (American
Samoa) (18).
Although STEPS metadata and microdata are available through the STEPS website or on request, the timeliness of analysis and
reporting varies across participating jurisdictions.
For USAPI jurisdictions participating in the USRDS, annual reports and a
web-based data repository are publicly available. USAPI mortality estimates, supported by the NVSS and WHO, are timely (ie, <4 y), with metadata and microdata available (5,6). USAPI jurisdictions generate hospital discharge reports
that are available to jurisdiction health program administrators and planners, physicians, and others on request.
Additionally, the WHO Western Pacific Office and Secretariat of the Pacific Community (SPC) provide web-based links to
current country health profiles (19) and the Pacific Regional Information System
databanks (20) for each USAPI jurisdiction. The WHO databanks,
updated annually, contain mostly crude data supplied by jurisdictions or
compiled from national surveys, reports, policy documents, and databases. The
PRISM databank links to jurisdiction statistical websites and provides regional
data tables. However, data availability, coverage,
and reliability vary from jurisdiction to jurisdiction and for each reported
measure. For example, FSM and RMI are the sole jurisdictions that link (PRISM)
to detailed reports related to mortality and hospital discharge summaries (20).
Integration
Overall, integration of available surveillance reports by USAPI chronic disease teams was rated as adequate across jurisdictions. For example, jurisdictions have used surveillance reports to develop a multiyear plan (2009-2013) supported by CDC for the integration of tobacco
control and diabetes prevention and control programs, although the incorporation of available population-based data is generally more extensive than for institution-based chronic disease data sources. The USAPI are
linking the multiyear plans for integrated tobacco control and diabetes prevention and
control with other NCD prevention initiatives to establish holistic approaches, decrease program overlap, and leverage resources within the islands.
CNMI, FSM, Palau, and RMI, with support from WHO and SPC, have developed national NCD plans (2008-2011), focused on reducing behavioral risk factors (eg, tobacco and alcohol use, dietary behaviors, and physical inactivity). American Samoa and Guam began development of national NCD plans in 2010, linking a number of healthy lifestyle initiatives (eg,
Live Healthy Guam) (21) and comprehensive cancer control plans: Guam Comprehensive Cancer Control Plan (2007-2012) and American
Samoa Cancer Prevention Plan (2001-2012) (9). Because most of the USAPI NCD multiyear plans were developed within the last 2 to 3 years, use of surveillance data in program evaluation was not assessed.
Back to top
Discussion
Our review showed that the USAPI jurisdictions are using both population-based and institution-based data sources
to build capacity for chronic disease surveillance. The USAPI chronic disease data sources are aligned with widely accepted indicators for chronic disease surveillance (11) that use standardized measures and methodology to collect, analyze, and report data related to chronic disease behavioral risk, preventive practices, illness, and death. Consistent use of these data
sources allows the USAPI to establish population benchmarks, compare chronic disease trends regionally and among other population groups within the United States and internationally, set priorities for resource allocations, and guide evidence-based policy and population health interventions needed for chronic disease prevention.
However, the review also illustrated the need to strengthen USAPI chronic disease surveillance through expanded support for valid and reliable data collection, analysis, and reporting among population-based data sources. For example, 5 jurisdictions began monitoring and tracking health risk behaviors among youth and young adults (YRBSS, YTS) in the early 1990s. Although these surveys are administered at standard intervals, statistical analysis and reports are generated by CDC for
participating jurisdictions that obtain an overall response rate of 60% or more and submit appropriate survey documentation. With the exception of Palau’s YRBSS, timely and reliable data collection representative of the target YRBSS youth and young adult population across survey years varies among participating jurisdictions. Similar challenges exist with obtaining representative samples every 4 to 5 years for the YTS
and GYTS.
Additionally, Guam, through participation in BRFSS, is the sole jurisdiction with sustained capacity for monitoring and tracking adult (≥18 y) health risk behavior and preventive practices.
Other jurisdictions (eg, Palau) are building capacity for participation in BRFSS or STEPS (American Samoa, CNMI, FSM, and RMI),
but financial resources and organizational capacity are limited. These constraints were particularly evident for STEPS, resulting in challenges with timeliness and
consistency of survey administration (>5 y in American Samoa and RMI), data analysis (ie, standardized weighting and disaggregation by age, sex,
and socioeconomic status), and reporting. USAPI jurisdictions’ chronic disease
surveillance infrastructure does not adequately support the standard
and complex analysis of STEPS and other available surveillance data.
Although jurisdictional institution-based chronic disease data sources use nationally accepted standards and methodology, data quality concerns remain. These concerns
are
- Timeliness of data collection, analysis, and reporting.
- Underreported vital statistics registration data.
- Underreported diagnostic or mortality data for USAPI residents who
receive medical treatment in the US mainland.
- Systematic biases in diagnosis by
health care providers in islands or atolls
with limited medical support.
- Health record system issues that include challenges with broadband
Internet access, lack of electronic medical record systems, lack of synthesis or analysis across multiple record systems, incorrect or incomplete death certificates, misinterpretation of ICD rules, and variations of coding categories for unknown and ill-defined diseases or cause of death (5,6,14).
Finally, this review did not assess biases within population-based data sources. For instance, the YRBSS and YTS exclude youths not attending or registered within jurisdictional school systems. The BRFSS includes only households with an available landline telephone and uses self-reported data. Additionally, sample size in some survey modules may limit data analysis. Lastly, responders to population health surveys might not be representative of the
total target population.
Back to top
Conclusion
Chronic disease surveillance can provide a foundation for population
health efforts designed to address health disparities within USAPI
communities. Using the HMNF, this assessment
provides an initial platform to understand the quality of existing USAPI
data sources and identify jurisdictional capacity for chronic disease
surveillance. The need to strengthen USAPI chronic disease surveillance
through continued assessment and expanded support for valid and reliable
data collection, analysis and reporting, dissemination, and integration
among population-based and institution-based data sources is common across
jurisdictions. Continued engagement of USAPI leadership across multiple
sectors (eg, public health, business, education, faith- and community-based
groups) to empower innovative systems and linkages for chronic disease
surveillance is essential for understanding and improving health
within Pacific communities.
Our recommendations are aligned with the White House Initiative on Asian
Americans and Pacific Islanders (www.whitehouse.gov/administration/eop/aapi)
and the Department of Health and Human Services (HHS) National Partnership
for Action to End Health Disparities (www.minorityhealth.hhs.gov/npa/)
designed to mobilize a comprehensive, community-driven, and sustained
approach to reducing health disparities among racial and ethnic minorities.
Recommendations include continued assessment, investment, and technical
assistance in support of a chronic disease surveillance system that
integrates USAPI population-based and institution-based data sources.
Innovative strategies that link and expand these data sources could advance
evidence-based policy and environmental transformations that target chronic
disease prevention. Related recommendations include 1) collaboration among USAPI governance, local and regional partnerships, and US and international
agencies to integrate surveillance; 2) investments to strengthen USAPI
infrastructure that support an expanded surveillance system; 3) workforce
development, through education and training, to promote quality
surveillance; and 4) translation of data to inform policy, research, and program planning and
evaluation at local, national, and international levels.
Back to top
Acknowledgments
We thank the following Pacific Island representatives who contributed to this project: Tuiasina Salamo Laumoli, Dottie Siavii, and Pasa Turituri, American Samoa; Joseph K. Villagomez, Rebecca Ann Covarrubias, Isidro Ogarto, John Tagabuel, Commonwealth of the Northern Mariana Islands; Vita A. Skilling, Marcus Samo, Shra Alik, and Brenda Hadley Eperiam, Federated States of Micronesia; J. Peter
Roberto, Roselie Zabala, and Gil S. Suguitan, Guam; Amenta Matthew, Justina Langidrik, Donny Andrike, and Godfrey Waidubu, Republic of the Marshall Islands; Augusta Rengiil, Republic of Palau. We also recognize the contributions of Lawrence Barker, Kaetz Beartusk, Michelle Carlberg, Gloria Colclough, Jack Colbert, Ed Gregg, Ann Goding, Laura Kann, Juliette Lee, Veronica Lea, Kristen McCall, Barbara Park, Karen Siener, Castine Verrill, Charles Warren, and MaryBeth Welton,
Centers for Disease Control and Prevention; and Susan Tanner, End-Stage Renal
Disease Network 17. Finally, we thank Nia Aitaoto and Dorraine Watts for their support and encouragement during this project.
Back to top
Author Information
Corresponding Author: Gwen Hosey, MS, ARNP, CDE, Centers for Disease Control and Prevention, 4150 Technology Way, Ste 210, Carson City, NV 89706. Telephone: 775-684-5907. E-mail:
ghh0@cdc.gov. Ms Hosey is a doctoral student at the Uniformed Services University of the Health Sciences, Bethesda, Maryland.
Author Affiliations: Henry Ichiho, Papa Ola Lökahi, Pacific Diabetes Education Program, Honolulu, Hawaii; Dawn Satterfield, Centers for Disease Control and Prevention, Atlanta, Georgia; Irene Dankwa-Mullan,
National Institute on Minority Health and Health Disparities, Bethesda, Maryland; Stevenson Kuartei, Ministry of Health, Koror, Republic of Palau; Kyu Rhee, Health Resources and Services Administration,
Rockville, Maryland; Tayna Belyeu-Camacho, Saipan, Commonwealth of the Northern Mariana Islands; Ione deBrum,
Diabetes Prevention and Control Program Coordinator, Republic of the Marshall Islands; Yorah Demei, Noncommunicable Disease Administrator, Koror, Palau; Kipier Lippwe, Noncommunicable Disease and Lifestyle Program Manager, Palikir, Pohnpei, Federated States of Micronesia; Patrick Solidum Luces,
Diabetes Prevention and Control Program Coordinator, Hagatna, Guam; Faiese Roby,
Diabetes Prevention and Control Program Coordinator, Pago Pago, American Samoa.
Back to top
References
- Preventing chronic disease: a vital investment.
World Health Organization; 2005. http://www.who.int/chp/chronic_disease_report/contents/en/index.html. Accessed
March 11, 2011.
- Kuartei S.
Managing health care systems in small island countries: Palau. Pac Health Dialog 2006;13(2):143-50.
- Ahmad OB, Boschi-Pinto C, Lopez AD, Murray CJL, Lozano R, Inoue M. Age standardization of rates: a new WHO standard. World Health Organization; 2001.
http://www.who.int/healthinfo/paper31.pdf. Accessed
March 11, 2011.
- Anderson RN, Rosenberg HM.
Age standardization of death rates: implementation of the year 2000 standard. Natl Vital Stat Rep 1998;47(3):1-16, 20.
- Xu J, Kochanek KD, Murphy SL, Tejada-Vera B. Deaths: final data for 2007. National vital statistics
reports 2010;58(19). National Center for Health
Statistics. http://www.cdc.gov/nchs/data/nvsr/nvsr58/nvsr58_19.pdf.
Accessed April 4, 2011.
- WHO Statistical Information Systems (WHOSIS). Mortality and burden
of disease statistics. Disease and injury country estimates (2004).
World Health Organization.
http://www.who.int/healthinfo/global_burden_disease/estimates_country/en/index.html.
Accessed April 4, 2011.
- Pacific partnerships for health: charting a course for the 21st century. Institute of Medicine.
http://www.nap.edu/openbook.php?record_id=5941. Accessed March 11, 2011.
- Hosey G, Aitaoto N, Satterfield D, Kelly J, Apaisam CJ, Belyeu-Camacho T, et al. The culture, community, and science of type 2 diabetes prevention in the US Associated Pacific Islands. Prev Chronic Dis 2009;6(3).
http://www.cdc.gov/pcd/issues/2009/jul/08_0129.htm.
Accessed March 11, 2011.
- Pacific countries and territories take up the battle against NCDs. Secretariat of the Pacific Community. Noumea
(NC); 2009. http://www.spc.int/hpl/index2.php?option=com_content&do_pdf=1&id=26. Accessed
March 11, 2011.
- Pacific Island Health Officers Association (PIHOA) Board Resolution 48-01. Declaring a regional state of health emergency due to epidemic of non-communicable diseases in the US Pacific Islands. 48th Annual PIHOA meeting. American Samoa; 2010.
http://www.pacifichealthvoices.org/files/PIHOA%20Resolution%2048-01%20NCD%20Emergency%20Declaration.pdf.
Accessed March 11, 2011.
- Centers for Disease Control and Prevention, Council of State and Territorial Epidemiologists, Association of State and Territorial Chronic Disease Program Directors.
Indicators for chronic disease surveillance. MMWR Recomm Rep 2004;53(RR11):1-6.
- Framework and standards for country health information systems. World Health Organization. 2nd edition. http://www.who.int/healthmetrics/documents/hmn_framework200803.pdf. Accessed
March 11, 2011.
- Haddock RL.
Disease surveillance in Guam: a historical perspective. Pac Health Dialog 2005;12(2):121-6.
- Tsark JU, Braun KL; Pacific Islands Cancer Council.
Reducing cancer health disparities in the US-associated Pacific. J Public Health Manag Pract 2007;13(1):49-58.
- Tsark JU, Braun KL, Palafox NA, Finau SA, editors. Cancer in the Pacific. Pac Health Dialog 2004;11(2):17-77.
- NCD risk factors STEPS report-2002. Federated States of Micronesia (Pohnpei).
http://www.who.int/chp/steps/STEPS_Report_Micronesia.pdf. Accessed March 11,
2011.
- NCD risk factors STEP report-2002. Republic of the Marshall Islands.
Majuro, Marshall Islands: Ministry of Health; 2007.
- America Samoa NCD risk factors STEPS report-2004.
http://www.who.int/chp/steps/Printed_STEPS_Report_American_Samoa.pdf. Accessed
March 14, 2011.
- Country health information profiles. World Health Organization,
Regional Office Western Pacific Region. http://www.wpro.who.int/publications/PUB_9789290614913.htm. Accessed
March 14, 2011.
- Pacific Regional Information System. Secretariat of the Pacific
Community. http://www.spc.int/prism/reports. Accessed
March 14, 2011.
- Live Healthy Guam. Guam Department of Public Health and Social Services. http://www.livehealthyguam.org/index.htm.
Accessed March 14, 2011.
Back to top
