
|
|
Volume 2: No.
4, October 2005
ORIGINAL RESEARCH
Trends in Walking for Transportation in the United States, 1995 and 2001
Sandra A. Ham, MS, Caroline A. Macera, PhD, Corina Lindley, MPH
Suggested citation for this article: Ham SA, Macera CA, Lindley C.
Trends in walking for transportation in the United States, 1995 and 2001. Prev
Chronic Dis [serial online] 2005 Oct [date cited]. Available from: URL:
http://www.cdc.gov/pcd/issues/2005/
oct/04_0138.htm.
PEER REVIEWED
Abstract
Introduction
The purpose of this study was to examine trends in walking for transportation
among U.S. adults and youth for Healthy People 2010
objective 22-14. The objective calls for increasing the proportion of trips of
1 mile or less made by walking to 25% for adults and 50% for youth. National
transportation surveys are used to track national health objectives, but data
interpretation and caveats to use have not been discussed in the public health
literature to date.
Methods
Cross-sectional analyses at two time points used data from the 1995
Nationwide Personal Transportation Survey and the subsequent 2001 National
Household Travel Survey. The populations of interest were U.S.
civilian noninstitutionalized adults (aged 18 years and older) and youth (aged 5 to 15
years). Trends were reported for the percentage of walking trips of 1 mile or
less for transportation (adults) and walking trips of 1 mile or less to school
(youth) using 86,286 trips (1995) and 119,462 trips (2001) made by adults and
3114 trips (1995) and 4073 trips (2001) made by youth.
Results
Of trips of 1 mile or less, adults reported more walking in 2001 (21.2%;
95% confidence interval [CI], 20.5–21.9) than in 1995 (16.7%; CI, 15.9–17.5).
For trips to school of 1 mile or less, youths also increased walking from 1995
(31.3%; CI, 27.9–34.4) to 2001 (35.9%; CI, 33.0–38.8). Changes in survey
methodology affected the interpretation of the Healthy People 2010
trends.
Conclusion
In spite of small increases in walking between 1995 and 2001 accompanying a
change in survey methodology, U.S. adults and youth fall short of meeting Healthy
People 2010 walking objectives for trips of 1 mile or less.
Back to top
Introduction
Regular physical activity decreases risk for many health conditions,
including cardiovascular disease, diabetes, colon cancer, and osteoporosis;
assists in weight control; and reduces symptoms of anxiety and depression (1).
Current recommendations encourage adults to engage in moderate-intensity
physical activity for at least 30 minutes on most, if not all, days of the
week for overall health (1,2). In 2001, less than one half of the U.S. adult
population reported reaching recommended levels of physical activity (3).
Although recent trends in leisure-time inactivity show some improvement, about
one quarter of adults reported no physical activity in their leisure time in
2002 (4). Only about one quarter of adolescents in grades 9 through 12 reported at
least 30 minutes of moderate-intensity physical activity on at least 5 days of
the week in 2001 (5). Moderate-intensity physical activity, such as walking,
has positive health effects, even when the purpose of walking is for
transportation rather than for exercise (1,6). Walking is the most commonly
reported physical activity among the general population; it is an activity
that most people can do, and it is low cost (7).
Healthy People 2010 objective 22-14 calls for adults and children to
walk more frequently for transportation. The target of the objective is for
adults aged 18 years and older to make 25% of their trips of 1 mile or less by walking and for
youth aged 5 to 15 years to make 50% of their trips to school of 1 mile or less by walking
(8). The baseline data for tracking these objectives were obtained from the
1995 Nationwide Personal Transportation Survey (NPTS), a survey that has been
conducted by the U.S. Department of Transportation since 1969 to track travel
and vehicle use patterns. Meanwhile, the most recent data on the
prevalence of walking for transportation can be found from the 2001 National
Household Travel Survey (NHTS) which combines two surveys that were conducted
separately in 1995 (i.e., the NPTS and the American Travel Survey of
long-distance trips). Estimates of the change in the prevalence of walking for
transportation between 1995 and 2001 for Healthy People 2010 objective
22-14 was determined for U.S. adults and youth from the 1995 NPTS and the 2001
NHTS. However, a public health analysis of walking for transportation has not
been published to date. This report expands upon Healthy People
objective 22-14 data on trends with additional demographic and environmental
correlates of walking for transportation among U.S. adults and youth. The
report includes a discussion of caveats to interpretation (e.g., question
design, analytical methodology, comparability across surveys) of Healthy
People 2010 trends and other public health and transportation analyses
that use this data.
Back to top
Methods
Surveys
The NPTS is a cross-sectional survey of personal transportation by the
civilian, noninstitutionalized population in the United States. From May 1995
through July 1996, 409,025 travel trips were reported by 95,360 people aged 5
through 88 in 42,033 households using 24-hour travel diaries (9). Households
were randomly selected from a list-assisted telephone number sample. All
household members aged 5 and older were asked in an initial household
interview to complete travel diaries for a randomly assigned day and to report
back in a follow-up telephone interview. Diary questions asked for trip
distance (miles or blocks), destination, mode of travel, start time, duration,
and identification of travel companions who lived in the household. Adult
proxies were used for youth younger than 14 years. Institutional Review
Board approval was obtained by the survey contractor, Research Triangle
Institute. The overall response rate to the initial interview, follow-up
interview, and diary was 34.3%; 92.2% of people in interviewed households
provided complete diary interviews (9).
In the survey, walking trips were defined as those for which “walk” was
the reported main travel mode, and trips to school were defined as all trips
with a destination of “school.” Trips were classified by five urbanization
categories (urban, second city, suburban, town, and rural) based on the
classification of the census block group in which the respondent’s household
was located (10). Second cities were secondary population centers located in
urbanized areas. Trips were the unit of analysis for the Healthy People
2010 objective; consequently, for this study we analyzed 86,286 trips of 1
mile or less made by adults aged 18 years and older and 3114 trips to school
of 1 mile or less made by children aged 5 to 15 years. Only trips with
complete travel distance, mode, purpose, and demographic information were
included in the analyses; trips with missing data were excluded.
The NHTS is a survey of personal transportation by the civilian,
noninstitutionalized population in the United States. From March 2001 through
July 2002, 642,292 travel trips were reported for 160,758 people from infancy
through 88 years of age in 69,817 households using 24-hour travel diaries
(10). The sample design and survey protocol were the same as described for the
1995 NPTS, except that children under 5 years of age were included in the
sample, and adult proxies were requested for youth aged 14 and 15 in 2001.
Diary questions and prompts were modified in 2001 to improve underreporting of
walking and bicycle trips (10); details of the diary changes can be found in
the Appendix. Institutional Review Board approval was obtained by the survey
contractors, Westat (Rockville, Md) and MORPACE International, Inc (Farmington
Hills, Mich). The overall response rate was
29.4%; 91.4% of people in interviewed households provided complete diary
interviews (10). For this study, we analyzed 119,462 transportation trips of 1
mile or less by adults and 4073 trips to school of 1 mile or less by children
aged 5 to 15 years. The operational definitions of walking trips, urbanization
classifications, and exclusion criteria were the same as for the NPTS 1995.
Additionally, of the 36 trip purpose categories, the three categories of 1)
“go to gym/exercise/play sports,” (2) “other social/recreational,” and
(3) walking trips for “pet care: walk the dog/vet visits” were considered
to be leisure-time activities (i.e., walking for exercise) and were
consequently excluded from the analysis (n = 8975).
Statistical analysis
The prevalence of walking trips for transportation of 1 mile or less was
reported separately for youth and adults by sex, family income, urbanization
classification, and geographic region, and for adults only by educational
attainment. The age-specific prevalence of walking trips was reported by sex
for youth and adults, and the prevalence of walking among adults by other
demographic characteristics was age-adjusted. Walking prevalence for youth and
adults by the nine U.S. Census divisions is shown on maps. Data were weighted
to adjust for survey nonresponse and selection bias and to represent all daily
travel made by all individuals in 1995 and 2001. Nonresponse adjustment
factors using U.S. Census population estimates for the survey years (e.g.,
age, sex, race/ethnicity, day of week, month, census region, household size, metroplitan area size) were applied to household then to person weights to obtain trip
weights. SUDAAN version 8.0 (Research Triangle Institute,
Research Triangle Park, NC) was used for statistical analyses, and ArcVIEW 3.2
(Environmental Systems Research Institute, Inc, Redlands, Calif) was used for
mapping.
Back to top
Results
On average, people in the United States made slightly more than four travel
trips per person per day in 2001. In 1995, 26.2% (23.9% in 2001) of all trips
among adults aged 18 and older were 1 mile or shorter (data not shown). Adults
made 21.2% of these short trips by walking in 2001, an increase from 16.7% in
1995 (Table 1). Trips made
by walking were least prevalent in 2001 among men aged 65 and older, rural and town residents, and residents of the South. The
percentage of walking trips by adults in 1995 and 2001 increased as residence
became more urban (8.7% of rural trips compared with 36.8% of urban trips in
1995, 14.0% of rural trips compared with 39.3% of urban trips in 2001) and had
a J-shaped relationship with education level with the highest prevalence of
walking among people with the lowest education (28.2% in 2001) and income
(29.1% in 1995, 38.5% in 2001) levels. The temporal trend for nearly all
categories was an increase in prevalence of as much as 9.4% among those with
family incomes of less than $10,000. Exceptions to this trend were in men and
women aged 65 and older, those with family income of $10,000–$19,999, and
urban residents. Trips made by walking were more common among adults living in
the Middle Atlantic, Pacific, and New England regions than among those living
in other regions (Figure 1).
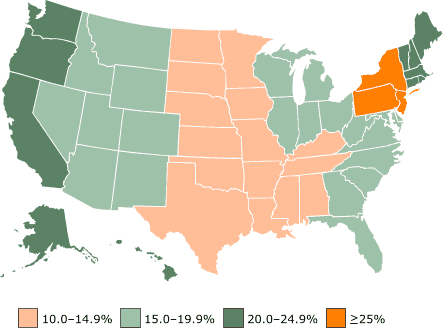
Figure 1. Walking trips of 1 mile or less made by
U.S. adults aged 18 years and older in 2001, by nine census divisions. [A
tabular version of this map is also available.]
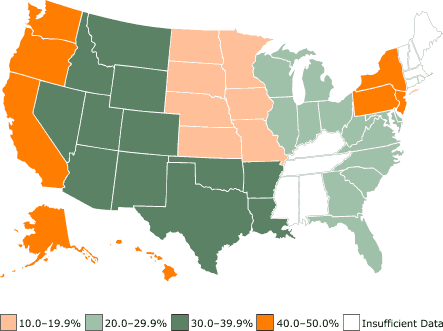
Figure 2.
Walking trips to school of 1 mile or less made by U.S. youth
aged 5 to 15 years in 2001, by nine census divisions. [A
tabular version of this map is also available.]
In 2001, of all trips to school made by children and adolescents aged 5 to
15, 36.2% were 1 mile or less in 2001, and 37.7% were 1 mile or less in 1995
(data not shown). Approximately 35.9% of these trips were made by walking in
2001, compared with 31.3% in 1995 (Table 2). In 2001, trips made to school by walking
were about the same among girls (36.6%) and boys (35.2%) and were more common
for the age group 10 to 15 years than for the age group 5 to 9 years. In both
1995 and 2001, walking to school was most prevalent in urban areas and in the
Northeast. The overall trend was no change from 1995 to 2001. Walking to
school increased among girls aged 10 to 15 years (29.9% in 1995, 42.5% in
2001), those with family incomes of less than $10,000 (35.0% in 1995, 54.5% in
2001), those with family incomes of $20,000–$34,999 (28.2% in 1995, 45.3% in
2001), and urban residents (43.5% in 1995, 62.4% in 2001).
Back to top
Discussion
Healthy People 2010 objective 22-14 calls for adults to make 25% of
their trips of 1 mile or less by walking and for children to make 50% of their
trips to school of 1 mile or less by walking (8). Although the percentages of
trips made by walking have increased since the 1995 baseline, 2001 data
suggest that, overall, U.S. adults and youth fall short of reaching this goal:
adults make only 21.2% of their trips of 1 mile or less by walking, and children
make only 35.9% of their trips to school of 1 mile or less by walking. These
analyses also found important differences in the prevalence of walking that
were related to environmental and demographic factors. Short trips are made by
walking more frequently by people who are younger than 30 years, have low
incomes, and live in urban areas or in the Northeast than by other
groups.
The travel diary incorporated methodological changes in 2001, including the
improved use of rosters of household members who traveled together, diary
prompts to record walking trips, and more detailed coding of transportation
activities (see Appendix). These changes were made to improve reporting and to
capture leisure-time walking in addition to transportation, and they resulted
in increased reporting of walking trips (10). Slight changes in question
wording in physical activity surveillance systems have been shown to affect
prevalence because physical activity behaviors are inherently difficult to
measure (11). Although the changes in survey questions and methodology were
intended to elicit better responses than in previous surveys (10), validation
studies for walking trips have not been published for 1995 or 2001
methodologies. It is likely that walking trips were underreported in 1995.
Because of changes in survey methodology, walking trips may have been more
accurately reported or overreported in 2001. Consequently, some of the
increases seen in walking for transportation may not be indicative of real
behavior change. The true increase from 1995 to 2001 was likely to be less
than these statistics suggest, but even if true, the prevalences are still
below the Healthy People 2010 targets for many groups. Nevertheless,
for more than 35 years these transportation surveys have captured travel and
physical activity behavior details that have not been available from public
health surveys. The third and final survey for Healthy People 2010
statistics for walking for transportation is anticipated in 2008.
Only about one third of children aged 5 to 15 traveled 1 mile or less to
school, and of these, 36% traveled by walking in 2001. The proportion of youth
who lived within 1 mile of school cannot be obtained from these data because
trips to school originated from home and other places. Walking to school is an
important source of physical activity for many children because of the low
percentage of children who take physical education in school (5) and the
popularity of sedentary leisure-time activities, such as watching television,
playing video games, and using the Internet. Participation in programs such as
the Centers for Disease Control and Prevention’s (CDC’s) KidsWalk-to-School is one way to increase physical activity and promote the
health of both children and adults (12). The increases in walking to school
among girls, those with family incomes of less than $35,000, and urban
residents may be the result of increased awareness of the importance of
walking to school through programs and media; however, causality cannot be
inferred from these cross-sectional data.
Low-income, low-education groups have a low prevalence of leisure-time
physical activity (1) and a high prevalence of multiple chronic disease risk
factors (13), although our results show that these groups have the highest prevalences of walking for transportation. Thus, it is important to measure
walking for transportation to assess lifestyle (e.g., leisure-time sports and
exercise, household, occupational, transportation-related) physical activity
levels. We do not know about black and Hispanic groups because race/ethnicity
questions were not asked of all survey respondents in 1995 or 2001. Large nonsignificant increases in prevalence in low-income groups and changes in
survey methodology to improve response rates and reporting of walking trips
suggest that those in low-income groups might have reported walking trips
differentially between the two surveys. The increases may also be due to the
impact of the Smart Growth movement, which has created more opportunities for
low-income families to live in walkable neighborhoods; active environments
promotional programs; and public health messages encouraging walking for
health benefits.
The choice to walk on short trips may be affected by time, purpose, or
environmental factors. These data show that walking for transportation is
related to the degree of urbanization for both children and adults. In urban
areas, schools, shopping, social and recreational opportunities, and
workplaces are more often integral parts of residential neighborhoods or are
more likely to be convenient to safe pedestrian routes and public transit.
Sprawling communities of newer suburban areas and second cities outside urban
cores were designed primarily for automobile transportation, separating
low-density residential neighborhoods from commercial, industrial, and office
spaces by roads with poor access between places (14). Urban design may be
reflected in the percentages of trips of 1 mile or less made by walking; in
2001, 39.3% of adults’ trips and 62.4% of youth's trips to school were made by
walking in urban areas, whereas lower percentages were found in second cities
and suburban areas. A recent study indicated that older women walked more
often if they lived within a 20-minute walk of a park, bicycle or walking
trail, or department, discount, or hardware store, and the trend for walking
increased with the number of destinations within walking distance (15). People who live
in neighborhoods with high walkability walked more than those
who lived in less-walkable neighborhoods (16). They also had lower rates of
obesity (16,17), lower health care costs, and increased longevity (17),
suggesting that environmental configuration may play a role. Additional
research is needed to determine how factors such as land use, sidewalks,
trails and parks, roads, and neighborhood safety relate to the urbanization
measure used for this report and how these design elements may be modified to
positively affect walking for transportation.
These Healthy People 2010 statistics may inform multidisciplinary
intervention strategies for health promotion. One recommended intervention
strategy is to increase access to places where people can be physically active
(18). For example, walking and bicycle trails that connect people with
existing social and commercial facilities would provide options to increase
physical activity.
One proposed framework for obesity prevention recommends using a set of
interventions selected for their level of promise (19). An intervention’s
promise would be assessed using a matrix based on the estimated population
impact and the level of certainty of the outcome. Using such a matrix
would ensure that interventions are considered that have a high potential
population impact but have less certainty of outcome. For example,
interventions that facilitate alternative modes of transportation (e.g.,
public transit, bicycling, walking) in suburban areas of a community may
not be economically justified because of “less promising” certainty of
effectiveness of increasing physical activity. Yet, the interventions may be
justified based on a highly promising potential of population impact and
reduction of the environmental and societal cost of automobile use (e.g., air
pollution, traffic congestion, and energy consumption) in a community with air
quality concerns and an ongoing Healthy Cities initiative.
This paper illustrates the need for understanding issues that may arise
from the multidisciplinary use of these survey data. Health surveys often
measure and report behaviors using “person” as the unit of analysis;
travel diaries can be analyzed at the person level and at the trip level.
Methodological differences (e.g., exclusion criteria based on physical
activity domain or missing data, age adjustment) may cause confusion about
differing prevalence statistics for apparently similar transportation
measures. For example, using the NPTS and NHTS, transportation researchers
reported that walking for transportation for all trip distances decreased from
9.3% in 1977 to 5.4% in 1995, then increased to 8.6% in 2001 (20). However, the
authors did not exclude walking for exercise from the analysis in 2001 nor did
they adjust for the changing age distribution in the U.S. over time. Another
reason why walking prevalence may vary across studies is that transportation
researchers often include all data in their denominators, whereas public
health researchers generally exclude observations with missing data. For
example, a similar study of walking prevalence by transportation researchers
included trips with incomplete data, resulting in lower prevalences than those
reported here (21).
The findings in this report are subject to at least five limitations.
First, data are cross-sectional and may not be used to infer cause and effect.
Second, the NHTS relies on self-reported information, which is subject to
recall bias that could decrease walking prevalence as well as social
desirability bias that could increase walking prevalence. However,
methodological changes were designed to improve reporting in 2001 (10). Third,
adults in each household reported trips made by children aged younger than 14
years in 1995 and younger than 16 years in 2001. Trip modes could have been misreported to
under- or overreport walking if adults did not accompany children to school.
Fourth, low response rates may have affected the representativeness of the
final study group because response rates vary by age, race/ethnicity, income
level, and other factors that could result in underreporting of travel in
socioeconomically disadvantaged groups (22). However, weighting for
nonresponse and selection bias used demographic, geographic, and temporal
measures. As expected, walking prevalence was highest in socioeconomically
disadvantaged groups. Finally, travel patterns may have been disrupted by the
events of September 11, 2001. The subsequent discovery of letters containing
anthrax that were sent to various recipients in several states from September
2001 to November 2001 may have decreased response rates because there was a
mail component of the survey (23).
Walking for transportation is part of an active lifestyle that is
associated with decreased risks for coronary heart disease (4), diabetes,
hypertension, and colon cancer and increased feelings of well-being (1).
Public health benefits could be gained with increased prevalence of walking
for transportation, using Healthy People 2010 objective 22-14 as a
guide (8). Walking for transportation is most prevalent in low-income and
low-education groups that have a high prevalence of multiple chronic disease
risk factors, including leisure-time physical inactivity (13). Methodological
changes in the surveys from 1995 to 2001 preclude a literal interpretation of
the trend statistics. Walking for transportation might have increased in youth
and adults because of concomitant trends of increasing popularity of walkable
communities to improve overall quality of life and promotion of walking,
active lifestyles, and walk-to-school programs to improve health. However, we
conclude that trend data for Healthy People 2010 indicate that most
youth and adults did not meet the objectives for walking for transportation in
2001, and the national travel surveys provide valuable data to the public
health community about active transportation. Changing a small percentage of
travel trips from automobile to walking could help people meet the levels of
physical activity set forth in Healthy People 2010 objectives.
Back to top
Author Information
Corresponding Author: Sandra A. Ham, MS, Health Statistician,
Physical Activity and Health Branch, Division of Nutrition and Physical
Activity, Centers for Disease Control and Prevention, Mail Stop K-46, 4770
Buford Hwy, Atlanta, GA 30341. Telephone: 770-488-5434. E-mail: sham@cdc.gov.
Author Affiliations: Caroline A. Macera, PhD, San Diego State University, San Diego, Calif;
Corina Lindley, MPH, Kaiser Permanente, Denver, Colo.
Back to top
References
- U.S. Department of Health and Human Services. Physical
activity and health: a report of the surgeon general. Atlanta (GA): Centers for Disease Control and
Prevention; 1996.
- Pate RR, Pratt M, Blair SN, Haskell WL, Macera CA, Bouchard C, et al.
Physical activity and
public health. A recommendation from the Centers for Disease Control and
Prevention and the American College of Sports Medicine. JAMA 1995;273(5):402-7.
- Centers for Disease Control and Prevention.
Prevalence of
physical activity, including lifestyle activities among adults — United
States, 2000-2001. MMWR 2003;52(32):764-9.
- Centers for Disease Control and Prevention.
Prevalence of no
leisure-time physical activity — 35 states and the District of Columbia,
1988-2002. MMWR 2004;53(4):82-6.
- Grunbaum JA, Kann L, Kinchen SA, Williams B, Ross JG, Lowry R, et al.
Youth risk
behavior surveillance — United States, 2001. MMWR CDC Surveill Summ 2002;51(4):1-62.
- Lee IM, Rexrode KM, Cook NR, Manson JE, Buring JE.
Physical activity and coronary heart disease in women:
is “no pain, no gain” passé? JAMA 2001;285(11):1447-54.
- Centers for Disease Control and Prevention. Participation in physical
activities. Atlanta (GA): Centers for Disease Control and Prevention; 1996.
Available from: URL: http://www.cdc.gov/nccdphp/dnpa/physical/ importance/index.htm.
- U.S. Department of Health and Human Services. Healthy People 2010:
understanding and improving health. 2nd ed. Washington (DC): U.S. Government
Printing Office; 2000 Nov.
- U.S. Department of
Transportation, Federal Highway Administration. User’s guide for the
Public Use Data Files: 1995 Nationwide Personal Transportation Survey.
Washington (DC): U.S. Department of Transportation; 1997.
- U.S. Department of Transportation, Federal Highway
Administration. 2001 National Household Travel Survey:
user’s guide. Washington (DC): U.S. Department of Transportation; 2004
Jun.
- Ham SA, Macera CA, Jones DA, Ainsworth BE, Turczyn KM.
Preliminary considerations for physical activity research: variations on a
theme. J Physical Activity and Health 2004;1:98-113.
- U.S. Department of Health and Human Services. KidsWalk-to-School: a guide to promote walking to school. Atlanta
(GA): Centers for Disease
Control and Prevention; 2000.
- Hayes DK, Greenlund KJ, Denny CH, Croft JB, Keenan NL.
Racial/ethnic and socioeconomic disparities in multiple risk factors for heart
disease and stroke — United States, 2003. MMWR 2005;54:113-7.
- Ewing R, Schmid T, Killingsworth R, Zlot A, Raudenbush
S. Relationship between urban sprawl and physical activity, obesity, and
morbidity. Am J Health Promot 2003;18(1):47-57.
- King WC, Brach JS, Belle S, Killingsworth R, Fenton M,
Kriska AM.
The relationship between convenience of destinations and walking
levels in older women. Am J Health Promot 2003;18(1):74-82.
- Saelens BE, Sallis JF, Black JB, Chen D.
Neighborhood-based differences in physical activity: an environment scale
evaluation. Am J Public Health 2003;93(9):1552-8.
- Pucher J, Dijkstra L.
Promoting safe walking and cycling
to improve public health: lessons from the Netherlands and Germany. Am J
Public Health 2003;93(9):1509-16.
- Centers for Disease Control and Prevention.
Increasing
physical activity. A report on recommendations of the Task Force on Community
Preventive Services. MMWR Recomm Rep 2001;50(RR-18):1-14.
- Swinburn B, Gill T, Kumanyika S.
Obesity prevention: a
proposed framework for translating evidence into action. Obes Rev
2005;6(1):23-33.
- Pucher J, Renne JL. Socioeconomics of urban travel:
evidence from the 2001 NHTS. Transport Q 2003;57:49-77.
- U.S. Department of Transportation, Federal Highway
Administration. 1995 Nationwide
Personal Transportation Survey. Washington (DC): U.S. Department of
Transportation; 1998.
- Cantor D, Shapiro G, Chen LW, Choudhry GH, Freedman M.
Nonresponse in the National Household Transportation Survey. Rockville (MD): Westat.
Available from: URL: http://trb.org/conferences/nhts/Shapiro.pdf*.
- Freedman M, Machado J, Swain S. Improving response
rates: methods employed to promote National Household Travel Survey
participation. Rockville (MD): Westat. Available from: URL: http://trb.org/conferences/nhts/Freedman.pdf*.
Back to top
*URLs for nonfederal organizations are provided solely as a
service to our users. URLs do not constitute an endorsement of any organization
by CDC or the federal government, and none should be inferred. CDC is
not responsible for the content of Web pages found at these URLs.
|
|
