
Sanitation Worker Run Over at Solid Waste Transfer Station--Virginia
FACE 9511
SUMMARY
On June 2, 1995, a 53-year-old male county garage service worker (the victim) died from multiple injuries after he was run over by a reversing front-end loader at a solid waste transfer station. The victim had been flagging refuse collection trucks into the tipping floor of a 10-bay solid waste transfer station. The front-end loader had just pushed refuse toward the tipping floor discharge openings and was backing out of the No. 4 bay in preparation to push refuse into the floor opening from the No. 3 bay. As the front-end loader backed out, the operator felt two bumps which he thought were trash bags. The end-loader operator stopped to reverse direction into the No. 3 bay; as he did so, he looked down in front of his machine and saw the victim lying on the pavement under the bucket. He immediately raised the bucket, dismounted and went to the victim, discovering that he had been run over. The operator went to the facility office and called 911. The EMS responded within minutes; however, the victim was dead at the scene. NIOSH investigators concluded that to prevent similar occurrences, employers should:
- ensure that mobile equipment is equipped with well- maintained audible backup alarms to warn pedestrians of impending equipment movement
- ensure that work procedures minimize or eliminate pedestrian exposure to hazards from moving vehicles and mobile equipment
- consider the use of sensing units to detect and warn mobile-equipment operators of the presence of pedestrians in the blind spots of mobile equipment
- consider providing personal audible alarms to pedestrian workers who are exposed to hazards of vehicle movement.
INTRODUCTION
On June 2, 1995, a 53-year-old male county garage service worker (the victim) died after being run over by a backing front-end loader while he was flagging refuse collection trucks at a solid waste transfer station. On June 23, 1995, officials of the Virginia Occupational Safety and Health Administration (VAOSHA) notified the Division of Safety Research (DSR) of the incident, and requested technical assistance. On July 6, 1995, a safety engineer and an engineering technician from DSR reviewed the case with the VAOSHA compliance officer assigned to the case and conducted an on-site investigation. During the investigation, the chief of operations for the County Division of Solid Waste Disposal and Resource Recovery was interviewed and photographs of the incident site were taken.
The transfer station in this incident was operated by the county and employed 135 workers, including 78 motor equipment operators. In addition to the victim, three other employees were routinely assigned duties of flagging traffic on a rotating basis.
The victim had worked for the county transfer station for 4 years. This was the first fatality at the transfer station, which began operations in January of 1982.
The county had a written safety policy which included a hazard assessment program that documented potential hazards for specific work areas and job locations at the transfer station. Flagging duties were not specifically listed; however, hazards of traffic movement at the tipping floor were noted and workers were warned never to turn their backs to oncoming traffic especially when flagging traffic.
INVESTIGATION
The incident occurred at a large county-owned solid waste disposal and recovery complex. This complex accepts, transfers, and recycles commercial and residential refuse. Part of the complex includes the transfer station where the incident occurred. Refuse collected throughout the county is brought to the transfer station by collection trucks, off-loaded and transferred to larger county-owned and -operated semi-trailer trucks, and transported to a county-operated resource-recovery facility and landfill. The county processes 870,000 tons of refuse annually.
The transfer station consists of a 178 foot by 123 foot maneuvering apron located in front (north) of a steel and brick building containing a lo-bay tipping floor, administrative offices and a scale house (Figure). Truck access to the open bay of the tipping floor is through 16-foot wide garage-type doors. Trucks are directed to a bay by a flagman.
Refuse is transferred from both county and privately owned collection vehicles by the following procedures. Collection vehicles are routed over the scales located at the east end of the building. As the vehicle comes off the scale, a flagman is stationed in front (North side) of the building near the columns between the garage doors, on the driver’s side of the door (right side facing the building). The vehicle proceeds to the door, swings to the North in the maneuvering area to square up with the door, and then backs onto the tipping floor under the flagman’s direction. Once the vehicle is positioned to dump, the flagman accepts the next vehicle off the scales, directing it in similar fashion.
While this is occurring, one or two front-end loaders push the refuse toward the South side of the building, where it falls into waiting semi-trailers located on a roadway under the floor. Hydraulic cranes, centrally located at the South edge of each floor opening, uniformly distribute the refuse in the semi- trailers for transport to the county generation/landfill facility. The tipping bay for each truck is determined by the amount and location of refuse on the tipping floor and the availability of semi-trailers, and is coordinated by visual communication among the crane operators, the front-end loader operators, and the flagman. The volume of material processed fluctuates weekly and daily, averaging 300 trucks daily, peaking with collection vehicle arrival rates of one per minute. The incident occurred during one of these peak periods.
Flagmen are instructed to remain as close as possible to the building columns, to minimize exposure to moving vehicles and/or equipment. Flagmen are directed never to turn their back to on- coming traffic. However, because of collection vehicles exiting or dumping in the bays between the flagman and the scale house, it may be necessary for the flagman to step out into the maneuvering area to make visual contact with the vehicle driver coming off the scale, returning to the front of column protectors after contact is established.
On the day of the incident, the front-end loader operator had just pushed material toward the floor opening in front of the No. 4 door, and was ready to egress into the maneuvering area and re-enter through the No. 3 door. As he was about to egress, a refuse-collection vehicle had just pulled off the scale and was traversing the maneuvering area in front of the doors. The front-end loader operator waited until the vehicle cleared the No. 4 door, checked the rear of his machine with the right and left mirrors, and backed out of the building. As he backed out, he felt two bumps as the loader ran over what he believed were trash bags. When he had cleared the building a sufficient distance to turn into the No. 3 door, he glanced down toward the front of the machine, and saw the victim lying on the pavement under the bucket. He immediately raised the bucket, dismounted and went to the office to call 911. The emergency medical service responded within 8 to 10 minutes; however, the victim was dead at the scene when they arrived.
CAUSE OF DEATH
The autopsy report listed the cause of death as multiple severe injuries.
RECOMMENDATIONS/DISCUSSION
Recommendation #1: Employers should ensure that mobile equipment is equipped with well-maintained audible backup alarms to warn pedestrian of impending equipment movement.
Discussion: The front-end loader in this incident was equipped with an audible alarm, which was activated when the machine’s transmission was shifted to reverse. According to the victim’s co-workers, the alarm was functioning correctly prior to the incident, however, when tested 2 hours after the incident, the alarm failed to operate. it could not be determined whether the alarm was operable at the time of the incident. Audible alarms which give warning when mobile equipment is reversing can provide warning to pedestrians even if out of sight of the equipment, allowing time for them to retreat from the vehicle’s path. This is especially important for work environments where more than one vehicle is operating.
Recommendation #2: Employers and operators of solid waste transfer facilities should ensure that work procedures minimize or eliminate pedestrian exposure to hazards from moving vehicles and mobile equipment.
Discussion: The procedure for routing trash collection vehicles at this transfer station requires that a flagman, (the victim) direct movement while standing in the maneuvering area of the vehicles. According to employer policy, the flagman is to remain in front of the building columns, between doors, and to always face oncoming traffic. These precautions were designed to place the flagman in an area where vehicles are unlikely to travel and to allow him to maintain visual contact with the driver of the collection truck. The flagman must accept each vehicle as it leaves the scale by establishing visual contact with the vehicle’s driver and indicating by hand signal the bay into which the vehicle is to back into and dump. The flagman must then remain near the building column on the driver’s side of the vehicle (right side facing building) while the vehicle is backed into the bay, to assure that the truck does not back into the discharge opening in the tipping floor. In doing this, he is required to face oncoming traffic. Given peak vehicle arrivals of one per minute, adherence to this procedure is difficult.
Several methods could be used to eliminate or reduce the hazards to pedestrians due to vehicle movement.
- Flagmen, scale operators, and front-end loader operators could be equipped with radios to eliminate complete reliance on visual communication, and the bays marked by lighted number signs. The decision as to which bay a truck is sent could be made through communication between the three workers, and the appropriate sign could be activated to direct the truck driver to the proper bay. This method could eliminate the need for the flagman to advance out into the maneuvering area to accept the truck as it leaves the scale, and allow him to remain proximate to the building column where contact between pedestrians and moving vehicles is less likely.
- The flagman could be stationed inside the administrative- office area of the building where he would have a view of the inside of the tipping building from a glass-enclosed office adjoining the tipping floor. From this location, he could activate a system of signal lights to indicate to the trash- collection vehicles which bay to tip in, while maintaining radio communication with the scale house and the front-end loader operators.
- Stop and go signal lights could be used to signal the truck drivers to stop backing in the bay. These signals could be operated manually by the flagman or automatically.
Recommendation #3: Employers should consider the use of sensing units to detect and warn mobile equipment operators of the presence of pedestrians in the blind spots of mobile equipment.
Discussion: The front-end loader in this incident was equipped with an audible alarm to warn pedestrians of reverse vehicle movement. While this type of warning system can prevent injury by notifying pedestrians to move out of the way, it fails to alert equipment operators of the presence of pedestrians. Equippinq mobile equipment and vehicles with sensing units to detect the presence of pedestrians in the blind spot and warn both operator and pedestrian would provide an additional margin of safety.
Recommendation #4: Employers should consider providing personal audible alarms to pedestrian workers who are exposed to hazards of vehicle movement.
Discussion: Small hand-held gas-operated horns capable of generating 112 dB of sound would allow pedestrians to Warn vehicle operators of their presence within the blind spot of equipment such as front-end loaders. it could not be determined whether the victim in this incident was aware of the approaching front-end loader as there were no eye witnesses. Had he been aware of the oncoming machine and for some reason was not able to clear the area, it may have been difficult for him to warn the front-end loader operator. A shouted warning probably would not have been audible to the operator, who was located in an enclosed cab.
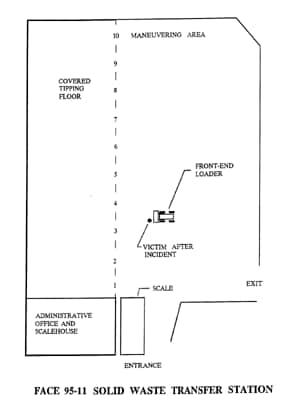
Figure.