
Volunteer Fire Fighter and Trapped Resident Die and a Volunteer Lieutenant is Injured following a Duplex Fire - Pennsylvania
 Death in the Line of Duty…A summary of a NIOSH fire fighter fatality investigation
Death in the Line of Duty…A summary of a NIOSH fire fighter fatality investigation
F2008-06 Date Released: November 28, 2008
SUMMARY
On February 29, 2008, a 21-year old male volunteer fire fighter (the victim) and a 33-year old volunteer Lieutenant were injured during a structural fire. The fire fighters were attempting to locate and rescue a 44-year old female resident from a burning duplex. The fire fighters became trapped on the second floor when fire conditions deteriorated. The victim was rescued by the rapid intervention team (RIT) and both the victim and injured Lieutenant were transported to the hospital. The victim remained in critical condition for several days in the burn unit before succumbing to his injuries on March 5, 2008. The female resident of the structure did not survive the fire. Key contributing factors identified in this investigation include the lack of water supply, fire fighters advancing within the burning structure without the protection of a charged hoseline, inadequate training in defensive search tactics, non-utilization of thermal imaging camera by the search crew, lack of coordinated ventilation, size-up information about the structure was not relayed to fire fighters, and interior reports were not relayed to the incident commander.
NIOSH has concluded that, to minimize the risk of similar occurrences, fire departments should:
- be prepared to use alternative water supplies during cold temperatures in areas where hydrants are prone to freezing
- ensure that search and rescue crews advance or are protected with a charged hoseline
- ensure fire fighters are trained in the tactics of a defensive search
- ensure that fire fighters conducting an interior search have a thermal imaging camera
- ensure ventilation is coordinated with interior fireground operations
- ensure that Mayday protocols are developed and followed
- ensure the Incident Commander receives pertinent information during the size-up (i.e., type of structure, number of occupants in the structure, etc.) from occupants on scene and that information is relayed to crews upon arrival
- ensure that fire fighters communicate interior conditions and progress reports to the Incident Commander
- develop, implement, and enforce written standard operating procedures (SOPs) for fireground operations
Additionally;
- fire departments and municipalities should ensure that citizens are provided information on fire prevention and the need to report emergencies immediately
- building owners and occupants should install smoke detectors and ensure that they are operating properly
INTRODUCTION
On February 29, 2008, a 21-year-old male volunteer fire fighter (the victim) and a 33-year old volunteer Lieutenant were injured during a fire at a two-story duplex. The victim remained in critical condition for several days in the burn unit of a metropolitan medical center before succumbing to his injuries on March 5, 2008. On March 5, 2008, the U.S. Fire Administration notified the National Institute for Occupational Safety and Health (NIOSH) of this incident. On March 18-21, 2008, two safety and occupational health specialists from the NIOSH Fire Fighter Fatality Investigation and Prevention Program investigated this incident. The NIOSH investigators interviewed the officers and fire fighters of the volunteer departments involved in this incident. The investigators met with the State Fire Marshal, local law enforcement officials and the County 911 Dispatch Deputy Director. NIOSH investigators also reviewed witness statements, photographs and video of the fireground and the victim’s training records and death certificate. NIOSH contracted with a personal protective equipment (PPE) expert to evaluate photographs of the victim’s and injured Lieutenant’s PPE. The incident site was visited, measured and photographed. The NIOSH investigators returned April 28-May 1, 2008 to meet with the mutual aid department and other fire fighters and officers not available during the first visit.
Fire Department
- Station 95 – Incident Command Department. The volunteer department in command of this incident is comprised of 25 fire fighters. The department has two stations and serves a population of approximately 9,000 in a geographical area of three square miles.
- Station 85 – Mutual Aid Department. The victim and injured Lieutenant from this volunteer department were the search and rescue crew that became trapped in the burning structure. The department has one station and is comprised of 32 fire fighters. The department serves a population of approximately 4,500 in an area of about 26 square miles.
- Station 87 – Mutual Aid Department. This volunteer department served as the Rapid Intervention Team (RIT) during this incident. The department has one station, is comprised of 49 fire fighters, and serves a population of approximately 8,700 in a geographical area of 63 square miles.
- Station 77 – Mutual Aid Department. This volunteer department served as additional manpower during this incident and conducted water shuttle operations. This department has one station, is comprised of 22 fire fighters, and serves a population of approximately 2,000 in a geographical area of 40 square miles.
The volunteer fire departments involved in this incident are part of a regional fire service group under a county wide mutual aid agreement.
Training and Experience
The 21 year-old victim had been a volunteer fire fighter with this department for 5 years. The victim had completed over 300 hours of training in areas such as exterior and interior fire fighting, fireground support, pump operations, truck company operations, hazardous materials, vehicle operations, vehicle rescue, incident command system (ICS), and national incident management system (NIMS). These courses were sponsored through the local community college and the state fire academy. The victim had also participated in several live fire training sessions coordinated through the local community college and state fire academy.
The IC reportedly had attended fire training courses, but no training records were provided for review.
Equipment and Personnel
- Station 95 – Incident Command Department
Chief 95 (Incident Commander) via personally operated vehicle (POV)
Accountability Officer via POV
Engine 95 (officer and five fire fighters)
Engine 95-2 (officer and two fire fighters)
Squad 95 (officer and three fire fighters) - Station 85 – Mutual Aid Department assigned Search and Rescue
Engine 85 (fire chief, four fire fighters including the victim)
Engine 85-2 (officer and four fire fighters)
Squad 85 (captain and fire fighter) - Station 87 – Mutual Aid Department assigned RIT
Rescue 87 (fire chief and five fire fighters) - Station 77 – Mutual Aid Department assigned Fire Suppression
Engine 77 (officer and four fighters)
Brush 77 (fire chief and fire fighter)
Tanker 77 (officer and fire fighter)
Timeline
The timeline for this incident included the initial call to the 911 Dispatch Center at 0606 hours. Only the units directly involved in the operations preceding the incident are discussed in this report. The response, listed in order of arrival and key events, includes:
- 0606 hours
- 911 Dispatch received a hang-up call from residence and law enforcement dispatched to investigate.
- 0609 hours
- 911 Dispatch received a cell phone call from right duplex resident reporting a fire with entrapment.
- 0610 hours
- Station 95 and Ambulance 100 dispatched.
- 0611 hours
- Mutual Aid Stations 85 and 87 (RIT) dispatched.
- 0612 hours
- Law enforcement on scene and reported “working fire and confirmed entrapment.”
- 0612 hours
- Chief 95 marked enroute in his POV and “copied” law enforcement radio traffic.
- 0613 hours
- Chief 95 requests Station 95 to be dispatched again after no acknowledgement.
- 0614 hours
- Engine 95 assistant chief requested additional engine company from Station 77. Station 77 dispatched.
- 0616 hours
- Chief 95 arrived on scene and became the incident commander.
- Accountability Officer arrived on scene by POV.
- Engine 95 marked enroute.
- 0617 hours
- Engine 95-2 marked enroute.
- 0618 hours
- Engine 85 marked enroute.
- 0619 hours
- Rescue 87 marked enroute.
- 0620 hours
- Engine 95 arrived on the scene with heavy smoke and fire coming from 1st and 2nd floors of right duplex at “A-D” corner.
- 0621 hours
- Engine 85-2 marked enroute.
- 0622 hours
- Engine 85 arrived on scene (victim and injured Lieutenant).
- Engine 77 marked enroute.
- 0623 hours
- Engine 95-2 arrived on scene.
- 0624 hours
- Victim and injured Lieutenant made entry into left duplex as search and rescue team
- 0626 hours
- Engine 85-2 arrived on scene.
- 0629 hours
- Engine 77 arrived on scene.
- 0631 hours
- Rescue 87 arrived on scene to serve as the RIT.
- 0637 hours
- Engine 85 sounded air horn evacuation for 10 seconds.
- Note: The evacuation was ordered by the IC after running out of water.
- Accountability Officer performed accountability check via radio with no response from search team.
- 0638 hours
- Heavy black smoke and fire consumed 1st and 2nd floor of left duplex.
- Injured Lieutenant radioed, “Help! Help! Help! I’m trapped on the second floor! I’m near a window!”
- 0640 hours
- Injured Lieutenant stumbled out of front door and collapsed in front yard. He yelled ” …is trapped on second floor!”
- 0641 hours
- RIT made entry into the left duplex.
- 0643 hours
- RIT exited duplex with victim.
Personal Protective Equipment
At the time of the incident, the victim and injured Lieutenant were wearing the full array of personal protective clothing and equipment, consisting of turnout gear (coat and pants), helmet, Nomex® hood, gloves, boots, and a self-contained breathing apparatus (SCBA) with an integrated personal alert safety system (PASS). The victim and injured Lieutenant were equipped with a portable radio and the victim also carried a TNT tool. The structural fire fighting gear was compliant with the 2003 edition of NFPA 1971.
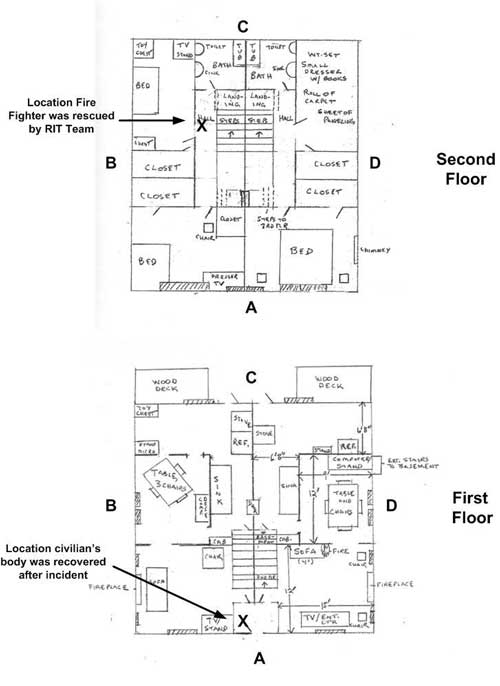
Structure
The incident structure was a two-story duplex originally built in the 1930s (see Photo 1 and Diagram 1). Each floor of the structure had approximately 1,088 square feet of furnished living area, with a 1,088 square foot unfinished basement. The structure was balloon-frame constructed and each unit of the duplex was a mirror image of the other. Each first floor had a living room, dining room and kitchen. There were two 40 square foot decks, one for each unit, at the rear of the structure and the units shared a common front entry. The second floors had two bedrooms and a bathroom. Interior construction was plaster over wood lath with carpeting over hardwood floors. The right unit had wood paneling throughout the first floor. Exterior construction was wood clapboards over wooden framing. The building owner had previously lived in the structure as a single family residence and had installed adjoining doors on the second floor and attic level in the 1960s. The building was not insulated and did not contain a rated fire wall between the units. The roof consisted of asphalt shingles and the house sat on a 75 x 75 foot level lot.
The cause and origin of the fire was ruled accidental by the State Fire Marshal, sparked by a hair dryer left running on the living room couch on the first floor right duplex. The occupants of the right unit (a husband and wife) had attempted to extinguish the fire with water prior to calling 911. The husband and wife had left the burning structure, but the wife went back to rescue their dog. The husband called 911 from his cell phone on the back porch and reported that his wife was trapped in the burning structure. The residents of the left unit safely evacuated. The structure was completely destroyed by the fire.
Weather
The weather at the time of the incident was partly cloudy with a temperature of 6°F and calm winds. The cold weather was a factor in this incident with two frozen hydrants in the vicinity of the structure.
INVESTIGATION
On February 29, 2008, at 0606 hours, the County 911 Dispatch received a hang-up call from a residence. Due to the 911 hang-up, local law enforcement was dispatched to investigate. At 0609 hours, County 911 Dispatch received a cell phone call from a duplex resident reporting a fire with entrapment. With law enforcement already enroute, the initial dispatch included Station 95 and ambulance 100 at 0609 hours. A second dispatch at 0611 hours included mutual aid Stations 85 and 87 (RIT).
Local law enforcement arrived on scene at 0612 hours and reported a working fire and confirmed entrapment with the building occupants who were outside the structure. Chief 95, the Incident Commander (IC), was marked enroute at 0612 hours and copied the law enforcement size-up. The Station 95 assistant chief heard this radio traffic while enroute to the station and requested an additional engine company from Station 77 which was dispatched at 0614 hours. The IC arrived on scene at 0616 hours by POV and the Accountability Officer followed immediately after, also by POV. Fire was showing from the first floor right unit with heavy fire on the second floor right unit. The IC did a quick 360° size up of the structure and determined the structure was a duplex by the two separate decks at the rear of the structure. (Note: During interviews, most fire fighters did not know that the structure was a duplex). The IC spoke to law enforcement and confirmed entrapment, but without a known location within the structure. Initial responding units were Engine 95 (E95) enroute at 0616 hours, Engine 95-2 (E95-2) enroute at 0617 hours, Engine 85 (E85) enroute at 0618 hours, Rescue 87 (R87) enroute at 0619 hours, Engine 85-2 (E85-2) enroute at 0621 hours, and Engine 77 (E77) enroute at 0622 hours. (Note: None of the fire fighters interviewed reported hearing a sounding smoke alarm).
Activities of Engine 95
E95 arrived on scene at 0620 hours and pulled just past the burning structure (see Diagram 2). They were instructed while enroute by the IC to perform fire suppression activities. Heavy smoke and fire was coming from the 1st and 2nd story windows on the right side of the house. The crew exited the engine and deployed the pre-connected 1 ¾” hoseline to the front door and a 2 ½” hoseline to the “A-D” corner. The crew checked in with the accountability officer and gave him their accountability tags. They started to flow water with the 1 ¾” hoseline from the common foyer but could not make entry into the right unit due to heavy fire conditions. Water was also being flowed at the “A-D” corner. (Note: No supply line had been established with a hydrant; thus the hose crews were operating from tank water). The officer vented a large window on the “A” side first floor of the left unit to let smoke out. The officer looked in this window and did not see the civilian victim, but noticed that the ceiling light was still on. E95 members, under the supervision of their officer, supplied a second 1 ¾” line to the search crew (victim and injured Lieutenant) at this same window after they made entry through it for a primary search. The E95 officer noticed that the search crew had finished their search on the first floor and were advancing to the second floor. He then placed a ladder to the second floor on the “A” side and broke the window out at the “A-B” corner (see Photo 2). He stated that there was not much heat on the second floor because the plastic insulation on the window was not melted, but he did notice heavy black smoke beginning to bank down. After venting this window he descended the ladder because he noticed a loss in water pressure from hoselines being operated at the front entrance and “A-D” corner. Within minutes an air horn sounded for evacuation from the structure. The E95 officer then went to a “B” side window on the second floor after hearing radio traffic that the search crew could not find their way out and they were by a window. He broke out a second floor window to release more smoke and to see if he could get the search crew out. The injured Lieutenant exited the structure through the front door and advised fire fighters that the victim was on the second floor. The RIT (R87) made entry at this time and rescued the victim.
Activities of Engine 95-2
E95-2 arrived on scene at 0623 hours and pulled directly behind E95 seeing heavy fire from the “A-D” corner. The operator drove past a hydrant looking for one closer to the fire scene. He did not see one near the fire scene and backed up the street to the hydrant he had originally passed. While doing so, he was passed by E85. E95-2 laid about 400 feet of 4″ large diameter hose (LDH) from this hydrant back down to the fire scene. A 1¾” pre-connected hoseline was taken off the engine to aid in fire suppression. After laying this LDH it was determined that the hydrant would not open and was frozen. The crew tried a hydrant two houses down and across the street from the fire scene and it was frozen also. A hydrant was finally found 300 feet away and a 3″ supply line was hand drug from E95-2 to this hydrant. E77 then pumped from this hydrant to E85-2 which supplied E85 with water.
Activities of Engine 85 and Engine 85-2
E85 arrived on scene at 0622 hours with heavy fire and smoke showing from the “D” side and “A-D” corner. The IC requested a search and rescue team for the entrapped civilian victim. The victim and injured Lieutenant teamed up as the search and rescue team. E85 then supplied E95 with a 5″ LDH and supplied them with their tank water. Other crew members removed ladders from the engine and placed them to the “B” side of the structure. E85-2 arrived on scene at 0626 hours and saw fire coming through the roof of the structure. E85-2 parked on a cross street north of the incident. E85 received 4″, 5″, and 2½” supply lines from other apparatus on scene. Note: E95-2 supplied E85 with its’ tank water via a 4″ LDH and E85-2 ran out of tank water while supplying E85 via a 4″ LDH until a portable drop tank and water shuttle was established by T77. It is unknown where the 2½” supply line came from.
Activities of Engine 77 and Tanker 77
E77 arrived on scene at 0629 hours pulling in behind E85-2 briefly to drop off the officer and crew. The E77 operator was instructed to man a hydrant further down the street to supply E95-2. This made room for T77 to pull in behind E85-2 at 0642 hours. T77 placed a drop tank and established a water shuttle so they could provide water to E85-2. The officer and crew from E77 walked down to the scene and checked in with the Accountability Officer. They noticed heavy fire from the “A-D” corner and heavy smoke on the first and second floors of the left duplex unit. Two fire fighters from E77 stayed in the manpower pool and the E77 officer took one fire fighter with him. This team initially acted as a RIT until E87 arrived. Once E87 arrived on scene and took over RIT duties, the E77 crew was ordered to assist in obtaining a viable water supply. They removed kinks from a LDH laid to E85 from E85-2. (Note: E85-2 was only flowing tank water at this time). The team then assisted in procuring a positive pressure fan after speaking with the Accountability Officer. They noticed another team from E85 had already placed a fan on the front stoop of the structure fire. Note: The positive pressure fan was never turned on. Chief 85 then advised this team to gear up and prepare to be a second search team. Before making entry, they ran out of water and the evacuation was sounded from E85 at the IC’s request. Radio traffic was heard from the injured Lieutenant stating “we are trapped at second floor side ‘D’ window”. This team noticed that the house was completely engulfed with fire and black smoke. They ran to the “D” side and realized the injured Lieutenant meant “B” side. They ran down the “D”side then across “C” to the “B” side where they found a ladder to a second floor window. The officer climbed this ladder to see if he could find the trapped search team. He ascended the ladder while it was footed by his teammate. There was heavy black smoke coming from this window, but no fire. He straddled the window sill attempting to hear any movement, a PASS device, or voices. He banged on the window sill to possibly get a response from the interior search crew. He received no response so he attempted to use his TIC, but the unit apparently malfunctioned. (Note: This department had had problems with the TIC since it was purchased. It had been returned to the manufacturer because of the screen “going white or blank”. The other departments on this fire had purchased the same brand of TIC with no malfunctions, but their TICs were never used during this fire). At some point the officer heard what he believed was the RIT team making entry onto the second floor and rescuing the victim. A fire fighter on the ground came to the ladder he was working on and advised him that the victim had been removed from the structure. The officer then descended the ladder and assisted with preparing the victim and injured Lieutenant for transport.
Activities of Victim and Injured Lieutenant
When E85 arrived on scene the IC advised them that he needed a crew to perform a search and rescue for the trapped civilian. The victim and injured Lieutenant received orders from the IC and performed a walk around of the structure. A window on the left side of the A-side was broken out and laddered for entry into the first floor. The victim and injured Lieutenant climbed up the ladder into the first floor of the left duplex unit and performed a primary search. There was some fire present, so the officer from E95 passed a charged 1¾” hoseline through the window to the search crew. They knocked down the fire on the first floor, then left the hoseline and went upstairs to perform a left hand search for the trapped victim. (Note: They did not know that the civilian was trapped in the right duplex). Conditions at this point were light smoke with little heat on the first floor. It could not be determined how far away from the stairs the search crew was on the second floor. The Lieutenant’s air supply was at half and the victim was unsure how much he had left so they decided to back out. (Note: No low air alarms had sounded). Conditions rapidly changed within seconds to intense heat and fire. These changes were viewed from the exterior at the same time the IC was calling for an evacuation from the building due to insufficient water. (Note: Two fire hydrants in the vicinity of the structure were reported to have been frozen and water supply was only available from the engines’ tanks. The portable tank and water shuttle was not established until after the evacuation alarm was sounded). E85 sounded its’ air horn at 0637 hours for ten seconds. The Accountability Officer immediately asked for a personnel accountability record (PAR) check and the E85 search team did not respond.
With deteriorating conditions on the second floor, the injured Lieutenant became disoriented and separated from the victim. He radioed for help at 0638 hours. “Help! Help! Help! I’m trapped on the second floor!” The injured Lieutenant believed he then broke a window and radioed “I’m near a window!” Fire fighters ran to the side of the structure and attempted to rescue the Lieutenant with ladders. Heavy flames were now pushing out the first floor windows. The Lieutenant managed to find his way to the staircase; he stumbled down the stairs and out the front door. His bunker gear was smoldering and he collapsed in the front yard at 0640 hours. He told the other fire fighters that the victim was trapped on the second floor.
Activities of the Rapid Intervention Team (RIT)
E87 arrived on scene at 0631 hours and was assigned RIT duties. RIT members immediately prepared their gear and tools needed for a potential rescue. The RIT members were placing ladders to exterior windows when they heard the air horn evacuation. They were in the front yard and heard the injured Lieutenant yelling that the victim was still inside the building at the top of the stairs on the left.
The RIT immediately donned their self-contained breathing apparatus (SCBA) and were comprised of Chief 87, and five fire fighters from R87, along with the Captain from Squad 85 who also had RIT training. A fire fighter from E85-2 grabbed a 1¾” hoseline and sprayed down the stairs in the common front foyer to allow the RIT team access and egress from the second floor. The R87 Chief reported that “the fire on the first floor was burning through the floor boards and the second floor was dark and smoky.
About 10 to 12 feet away from the top of the stairs on the left Chief 87 felt the victim’s boots. The victim was on his hands and knees, “not really moving, in kind of a fetal position, he was moaning, in and out of it.” (Note: The victim’s PASS devise did not activate. It is believed he was still moving.) As the RIT dragged the victim down the stairs, the 85 Captain stepped through the floor at the top of the stairwell but was not hurt. The victim and RIT exited the structure at 0643 hours.
Activities after the Rescue
The IC changed his fire attack approach to defensive immediately following the evacuation horn (see Photo 3). Fire fighters concentrated on protecting exposures and suppressing a vehicle fire caused by the collapse of the “D” side wall. A water shuttle was set-up to supply water for their defensive attack.
The trapped female resident did not survive the fire and was pronounced dead at the scene. Both the victim and injured Lieutenant were transported to an area hospital where they were stabilized. They were later transported to the burn unit of a metropolitan medical center where the injured fire Lieutenant was treated and released. The victim remained in critical condition before succumbing to his injuries on March 5, 2008.
Analysis of Bunker Gear worn by the Victim and Injured Lieutenant
Photographs of the victim’s and injured Lieutenant’s PPE were examined and analyzed by a personal protective clothing expert contracted by NIOSH. The analysis of the victim’s gear indicated that the gear had sustained an emergency type event (a flashover) as there was heavy charring on the shell of the gear and dye sublimation occurred on the interior side of the thermal barrier. This dye sublimation is uncommon except under the most extreme of circumstances. Since the fire fighters were quickly removed from the structure, it is highly likely that the victim was exposed to a flashover. There was less damage to the injured Lieutenant’s gear, but his proximity to the worst part of the flashover could have been different, or he might have been shielded from some of the effects given his specific position and orientation.
CONTRIBUTING FACTORS
Occupational injuries and fatalities are often the result of one or more contributing factors or key events in a larger sequence of events that ultimately result in the injury or fatality. NIOSH investigators identified the following items as key contributing factors in this incident that ultimately led to the fatality:
- Inadequate water supply. Two hydrants in the vicinity of the burning structure were frozen from the cold weather.
- The victim and injured Lieutenant did not have the protection of a charged hoseline during their search for the trapped occupant.
- Inadequate training in defensive search tactics.
- Non-use of a thermal imaging camera which may have allowed the search and rescue crew to advance more quickly through the structure.
- Ventilation was not coordinated with the interior search.
- Size-up information about the structure was not relayed to the interior search crew. The interior crew was searching in the wrong duplex for the trapped occupant and did not realize they were in a duplex.
- The incident commander was unaware of the search crew’s location in the building. He did not receive any interior reports and was concentrating on resolving water supply issues.
CAUSE OF DEATH
According to the county medical examiner’s office, the victim died 5 days after the incident due to complications from the thermal injuries he received to over 71% of his body.
FIRE FIGHTER INJURIES
The injured Lieutenant received thermal burns over 8% of his body.
RECOMMENDATIONS
Recommendation #1: Fire departments should be prepared to use alternative water supplies during cold temperatures in areas where hydrants are prone to freezing.
Discussion: Establishing adequate water supply on the fireground is an integral part of fire suppression. Regardless of the choice of attack method or the type of fire stream used, successful fire suppression depends upon discharging a sufficient quantity of water to remove the heat being generated, and ensuring that it reaches the fire rather than being turned into steam or being carried away by convective currents.1 During this incident, the fire departments involved attempted to deploy large diameter hoses (LDH) for a hydrant water supply line. Fire fighters were unable to open two of the hydrants in the vicinity of the incident structure. Fire fighters bent their hydrant wrench on one of the frozen hydrants (see Photo 4). These hydrants were checked and lubed twice a year by public works officials and opened freely several hours after the fire incident. Temperatures that morning were around 6°F, with several inches of snow on the ground. Fireground operations were mainly run from apparatus tank water; this caused fluctuations in water pressure and sometimes no water at all. The hydrants installed in this neighborhood were dry-barrel hydrants. Dry-barrel hydrants are routinely installed in geographical areas that are exposed to freezing conditions. Dry-barrel hydrants are still opened the same as wet-barrel hydrants, except that the main valve is located underground below the frost line. Once the dry-barrel hydrant is closed, the water in the barrel will drain out underground through drain holes.2 These drain holes remain open until the hydrant is opened again, allowing flow of water. It is believed that either the drain holes got clogged, not allowing water to drain out from a prior use, or that ground water from excessive rainfall found its way into the barrel via the opened drain holes and froze, rendering the hydrants inoperable. In preparation for potential issues, fire departments should develop standard operating procedures (SOPs) for temporary water sources to be dispatched like tankers, water shuttles, or portable drop tanks.
Recommendation #2: Fire departments should ensure that search and rescue crews advance or are protected with a charged hoseline.
Discussion: Fire departments should develop SOPs to ensure that a charged hoseline is either advanced with the search and rescue crew or is operated by another fire fighter providing the team with protection while entering hazardous or potentially hazardous areas containing fire. A fire fighter is taking a substantial risk when entering a burning structure without a charged hoseline or protection from one. The only justification for risking a fire fighter’s life is present when there is a real chance to save another person’s life.1 According to Dunn, the most important fire fighting operation at a structure fire is stretching the first attack hoseline to the fire.1, 3 A properly positioned and functional fire attack line saves the most lives during a fire.3 “It confines the fire and reduces property damage. Searches will proceed quickly, rescues will be accomplished under less threat, sufficient personnel will be available for laddering, ventilation will be effective, and overhaul above the fire room will be unimpeded.” 1 During this incident, the victim and injured Lieutenant originally obtained a 1 ¾” hoseline to put out fire on the first floor of the left duplex unit they were searching. Once the search was complete and the fire was out they ascended to the second floor, but did not take the hoseline with them. Fire conditions rapidly changed as the fire from the right unit made its way into the left unit where they were searching. There were no other fire fighters or attack crews within the structure to provide protection to the search crew.
Recommendation #3: Fire departments should ensure fire fighters are trained in the tactics of a defensive search.
Discussion: As stated in Dunn’s Command and Control of Fires and Emergencies, “There are two warning signs that may precede flashover: heat mixed with smoke and rollover. When heat mixes with smoke, it forces a fire fighter to crouch down on his hands and knees. If you are forced down to the floor by intense heat, consider the possibility of flashover. As mentioned above, rollover presages flashover.”3 Whenever one of these danger signs exists, defensive search tactics must be used. Three defensive search tactics are as follows:
- At a door to a burning room that may flashover, fire fighters should check behind the door to the room and sweep the floor near the doorway. Fire fighters should not enter the room until a hose line is in position.
- When there is a danger of flashover, fire fighters should not go beyond the “point of no return.” The point of no return is the maximum distance that a fully equipped fire fighter can crawl inside a superheated, smoke-filled room and still escape alive if a flashover occurs. The point of no return is approximately five feet inside a doorway or window.
- “When searching from a ladder tip placed at a window, look for signs of rollover if one of the panes has been broken. If rollover is present, do not go through the window. Instead, crouch below the heat and sweep the interior area below the windowsill with a tool. If a victim has collapsed there, you may be able to crouch below the heat enough to pull him to safety.”
Fire fighters performing a search or interior attack should also be concerned with the danger of being trapped above a fire. This is greatly influenced by the construction of the burning building. Of the five basic building construction types (fire resistive, noncombustible, ordinary construction, heavy timber, and wood-frame), the greatest danger to a fire fighter who must search above the fire is posed by wood frame construction. Vertical fire spread is more rapid in this type of structure. Flames may spread vertically and trap fire fighters searching above the fire in four ways: up the interior stairs, through windows, within concealed spaces, or up the combustible exterior siding. During this incident, conditions changed very quickly. The officer from E95 noticed heavy dark smoke banking down on the first floor after the search crew continued their search to the second floor. The injured Lieutenant remembers reaching the second floor of the duplex and noticing low heat and dark smoke. Within seconds the room lit up disorienting the injured Lieutenant and severely injuring the victim. Fire fighters on the exterior reported seeing fire go from the right duplex into the left duplex in a matter of moments. (Note: This is about the time in the incident when fire fighters were without water). The injured Lieutenant was able to make it out, but the RIT had to rescue the victim from the second floor.
Recommendation #4: Fire departments should ensure that fire fighters conducting an interior search have a thermal imaging camera.
Discussion: A thermal imaging camera (TIC) is a highly valuable tool for assisting fire fighters in quickly getting crucial information about the location of the seat of the fire from the exterior of the structure. Knowing the location of the most dangerous and hottest part of the fire may help fire fighters determine a safe approach and avoid structural damage in a building that might have otherwise been unnoticeable. Ceilings and floors that have become severely weakened by fire damage and are threatening to collapse may be spotted with a thermal imaging camera. A fire fighter about to enter a room filled with flames and smoke can use a TIC to assist in judging whether or not it might be safe from falling beams, walls, or other dangers. The TIC can also be used during interior searches to help locate a missing fire fighter or civilian. Smoke can become heavy within a structure not allowing visibility. The use of a TIC may also provide additional information the Incident Commander can use during the initial size-up and ongoing fire attack decisions. TICs should be used in a timely manner and fire fighters should be properly trained in their use and be aware of their limitations.4
During this incident the victim and injured fire Lieutenant made entry into the left duplex through a window on the first floor “A” side. They received orders to conduct a primary search of the structure for a civilian victim. The civilian’s whereabouts were unknown to the IC and the search team. A TIC could have decreased the time needed to search the duplex, and could have alerted them to the deteriorating fire conditions around them from the fire’s progression through the balloon frame construction. They found themselves on the second floor with the inability to find a way out.
Recommendation #5: Fire departments should ensure ventilation is coordinated with interior fireground operations.
Discussion: Ventilation decisions should be part of the initial size-up and are necessary to improve the fire environment in order for fire fighters to approach a fire with a hoseline for extinguishment or to allow a quick search for any victims. Ventilation is performed to relieve the products of combustion, allowing fire fighters to advance on the fire. The ventilation needs to be coordinated as fire fighters progress through a structure fire. When venting, the principle is to pull the fire, heat, smoke, and toxic gases away from victims, stairs, and other egress routes.5 Coordinating ventilation with interior operations ensures that ventilation does not pose risks for fire fighters operating in the interior. By eliminating smoke, heat, and gases from the fire it will help minimize flashover conditions.2
In this incident, the IC had ordered the structure to be ventilated by arriving fire fighters by breaking out the exterior windows. The victim and injured Lieutenant had just finished performing a primary search on the first floor of the left duplex. (Note: The right duplex had heavy fire conditions and thick black smoke. The left and right duplex shared a common non-insulated and non-fire proof wall). They then proceeded up a set of stairs to perform a search of the second floor. They were without a TIC and hoseline. Fire conditions upon entering the second floor showed light smoke and a little heat. An evacuation from the structure was called due to water supply problems while windows on the second floor of the left duplex were being vented. Conditions rapidly changed to intense heat, fire, and smoke. The injured Lieutenant became disoriented and immediately called for help. Smoke filled the second floor and oxygen from the vented second floor windows aided in igniting the unburned fuel and pulling the flames towards the left duplex of the second floor around the victim and injured Lieutenant.
Recommendation #6: Fire departments should ensure that Mayday protocols are developed and followed.
Discussion: Fire fighters must act promptly when they become lost, disoriented, injured, low on air, or trapped.6-10 First, they must transmit a distress signal while they still have the capability and sufficient air. The next step is to manually activate their PASS device. To conserve air while waiting to be rescued, fire fighters should try to stay calm and avoid unnecessary physical activity. If not in immediate danger, they should remain in one place to help rescuers locate them. They should survey their surroundings to get their bearings and determine potential escape routes, and stay in radio contact with Incident Command and rescuers. Additionally, fire fighters can attract attention by maximizing the sound of their PASS device (e.g., by pointing it up in an open direction), pointing their flashlight toward the ceiling or moving it around, and using a tool to make tapping noises. A crew member who initiates a Mayday call for another person should quickly try to communicate with the missing member via radio and, if unsuccessful, initiate a Mayday providing relevant information as described above.
When a “MAYDAY” is transmitted the IC must either personally handle the situation or designate another officer to do so. Part of “handling” a Mayday is to communicate with the trapped or lost fire fighter(s) and with any other fire fighters or officers involved. A Mayday protocol can outline the fire ground response plan and duties of fire fighters, officers, dispatch center, and IC. This will hopefully reduce any confusion during the Mayday. During this incident, there were no SOPs established within the fire department or County 911 Dispatch on how to handle a “MAYDAY”. Resources were provided for a rescue, but no written policies. The injured Lieutenant radioed that he was lost on the second floor. The Accountability Officer could not verify the injured Lieutenant’s location within the structure. The radio traffic from the fireground continued and at times “walked over” radio transmissions from the injured Lieutenant causing a delay in response. Radio traffic should be halted by the IC or County 911 Dispatch allowing emergent or “MAYDAY” transmissions to be heard.
Recommendation #7: Fire departments should ensure that the Incident Commander receives pertinent information during the size-up (i.e., type of structure, number of occupants in the structure, etc.) from occupants on scene and that information is relayed to crews upon arrival.
Discussion: A proper size-up begins from the moment the alarm is received, and it continues until the fire is under control. Several factors must be evaluated in conducting the size-up, for example, the type of structure and its construction, occupants, time of day, contents of the structure, and potential hazards.1 During the size-up, the IC should attempt to determine the approximate location and intensity of the fire, how best to reach the seat of the fire, and the likely locations of civilian victims.
The County 911 Dispatch dispatched the fire as a single address. Upon arrival to the scene, the IC conducted a 360° walk around the structure and found two separate rear decks. He determined at this point that the structure was a duplex. He was unsure whether the duplex was set-up longitudinal or latitudinal. The residents of either unit were not available to tell the IC information about the structure. Local law enforcement had previous knowledge of the duplex type structure when they arrived before the IC, and they confirmed that a civilian was still trapped in the structure but the whereabouts of the civilian was unknown. The information about the trapped civilian was relayed to the incoming engine company assigned to search and rescue, but they were never made aware that the structure was a duplex. This information is invaluable when trying to determine where and how to search a structure or perform a fire attack. The civilian victim lived in the duplex unit on the right and it was believed she made entry back into the right duplex to retrieve her dog, but the search crew entered into the left unit to perform their primary search. Knowing that the victim was probably still in the right unit could have prevented the search crew from having to search the left unit since the occupants of the left unit were accounted for prior to their arrival.
Recommendation #8: Fire departments should ensure that fire fighters communicate interior conditions and progress reports to the Incident Commander.
Discussion: The size-up of interior conditions is just as important as exterior size-up. The IC is monitoring exterior conditions while the interior conditions should be monitored and communicated to the IC as soon as possible. Knowing the location and the size of the fire inside the building lays the foundation for all subsequent operations. Interior conditions could change the IC’s strategy or tactic.11 Also, when operating inside the structure, fire fighters should communicate to the IC when making initial entry, areas have been searched and cleared, progressing between floors, and when exiting the structure. During this incident, no radio communications took place between the search crew and IC. The search crew had a verbal face-to-face communication with the officer of E95 upon searching the first floor and before progressing to the second floor. Though the IC ordered a crew to perform search and rescue, their progress and position reports were never communicated to him.
Recommendation #9: Fire departments should develop, implement, and enforce written standard operating procedures (SOPs) for fireground operations.
Discussion: Written SOPs enable individual fire department members an opportunity to read and maintain a level of assumed understanding of operational procedures. Conversely, fire departments can suffer when there is an absence of well developed SOPs. The NIOSH Alert: “Preventing Injuries and Deaths of Fire Fighters” identifies the need to establish and follow fire fighting policies and procedures.12 Guidelines and procedures should be developed, fully implemented and enforced to be effective. Periodic refresher training should also be provided to ensure fire fighters know and understand departmental guidelines and procedures.
The following NFPA Standards also identify the need for written documentation to guide fire fighting operations:
NFPA 1500, Fire Department Occupational Safety and Health Program states that fire departments shall prepare and maintain policies and standard operating procedures that document the organizational structure, membership, roles and responsibilities, expected functions, and training requirements, including the following….(4) The procedures that will be employed to initiate and manage operations at the scene of an emergency incident (NFPA 1500).13
NFPA 1561, Standard on Emergency Services Incident Management System states that standard operating procedures (SOPs) shall include the requirements for implementation of the incident management system and shall describe the options that is available for application according to the needs of each particular situation (NFPA 1561).14
NFPA 1720, Standard for the Organization and Deployment of Fire Suppression Operations, Emergency Medical Operations, and Special Operations to the Public by Volunteer Fire Departments states that the authority having jurisdiction shall promulgate the fire department’s organizational, operational, and deployment procedures by issuing written administrative regulations, standard operating procedures, and departmental orders (NFPA 1720).15
At the time of the incident, the initial responding departments either had verbal or no written SOPs for fire fighters to review and follow. (Note: The incident command station is currently in the process of revising and putting in writing their SOPs for distribution to their members.)
Recommendation #10: Fire departments and municipalities should ensure that local citizens are provided with information on fire prevention and the need to report emergency situations as soon as possible to the proper authorities.
Discussion: One of the simplest and most effective methods of achieving the goal of the preservation of life and property is prevention. The importance of citizens reporting an emergency situation, as soon as possible, to the proper authorities cannot be overemphasized. Any delay allows the fire a chance to increase in intensity and spread. Brannigan states “make it clear that the fire department should be called if smoke is even smelled.16 This might indicate a hidden fire”. As stated in the Fire Fighter’s Handbook “teaching our citizens to recognize life safety hazards and to react appropriately is clearly a fire department function and responsibility”. 17 According to the Fire Marshals’ report, the fire started from a hair dryer that was running on the arm of a four foot sofa of unknown material. The civilian victim happened to be on the sofa when the fire started. She called for her husband who was upstairs. He came downstairs to see flames as high as two feet off the sofa, and went into the kitchen to find something to put out the fire. He came back to the sofa with a bucket of water and the sofa was fully involved and burning up the wall. He then exited from the rear of his duplex and called 911 on his cell phone. The civilian victim, his wife, entered back through the front entrance to retrieve their dog, but did not make it out. (Note: There was a 911 hang-up call recorded by the County 911 Dispatch from the duplex involved, but the phone was busy when attempting to call back).
Recommendation #11: Building owners and occupants should install smoke detectors and ensure that they are operating properly.
Discussion: A smoke detector is a life saving device that is installed in single-family residences and in smaller multi-family style occupancies.2 The purpose of a smoke detector is to sound an alarm or alert tone when it detects products of combustion from a fire in the room where it is installed. Having a smoke detector in a home can more than double someone’s chance of survival and this is important to understand since 80% of fire deaths occur in homes.18 Smoke detectors should be tested monthly and installed on all levels of a home to include sleeping areas, hallways, and common areas.
The house burnt to the ground and investigators were unable to determine whether or not the duplexes had smoke detectors. No smoke alarm or alert tone was heard by arriving units or County 911 Dispatch taking the occupants’ 911 call. Having a smoke detector in this incident would not have prevented the fire, but it may have alerted the residents to the fire more quickly, providing time for them to safely exit the residence. Building code officials in this jurisdiction are currently establishing a program to ensure that working smoke detectors are properly placed within a single or multi-family dwelling.
REFERENCES
- Dunn V [1992]. Safety and Survival on the Fire Ground. Saddle Brook, NJ: Fire Engineering Books and Videos.
- International Fire Service Training Association [2008]. Essentials of Fire Fighting, 5th ed. Stillwater, OK: Fire Protection Publications, Oklahoma State University.
- Dunn V [1999]. Command and Control of Fires and Emergencies. Saddle Brook, NJ: Fire Engineering Books and Videos.
- Corbin DE [2000]. Seeing is believing. Dallas, TX: Occupational Safety and Health, Aug 69 (8): 60-67.
- Klaene BJ, Sanders RE [2000]. Structural Fire Fighting. Quincy, MA: National Fire Protection Association.
- Angulo RA, Clark BA, Auch S [2004]. You Called Mayday! Now What? Fire Engineering, September issue.
- Clark BA [2004]. Calling a mayday: The drill.external icon [http://www.firehouse.com/article/10515446/calling-a-mayday-the-drill]. Date accessed: June 2008. (Link Updated 1/15/2013)
- DiBernardo JP [2003]. A missing firefighter: Give the mayday. Firehouse, November issue.
- Sendelbach TE [2004]. Managing the fireground mayday: The critical link to firefighter survival. [http://cms.firehouse.com/content/article/article.jsp?sectionId=10&id=10287]. Date accessed: August 2008. (Link no longer available 1/15/2013)
- Miles J, Tobin J [2004]. Training notebook: Mayday and urgent messages. Fire Engineering, April issue.
- Dunn, V. [1988] Collapse of Burning Buildings: A Guide to Fireground Safety. Saddle Brook, NJ: Fire Engineering Books and Videos.
- NIOSH [1994]. NIOSH Alert: preventing injuries and deaths of fire fighters. Cincinnati, OH: U.S. Department of Health and Human Services, Public Health Service, Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health, DHHS (NIOSH) Publication No. 94-125. [https://www.cdc.gov/niosh/fire.html]
- NFPA [2007]. NFPA 1500: Fire department occupational safety and health program. Quincy, MA: National Fire Protection Association.
- NFPA [2008]. NFPA 1561: Standard on fire department incident management system. Quincy, MA: National Fire Protection Association.
- NFPA [2004]. NFPA 1720: Standard for the organization and deployment of fire suppression operations, emergency medical operations, and special operations to the public by volunteer fire departments. Quincy, MA: National Fire Protection Association.
- Brannigan FL [1999]. Building construction for the fire service. Quincy, MA: National Fire Protection Association.
- Thomson Delmar Learning. Fire Fighter’s Handbook [2000]. Essentials of fire fighting and emergency response. New York: Delmar Publishers.
- National Safety Council [2005]. Home Fire Prevention and Preparedness.pdf iconexternal icon http://www.nsc.org/Membership%20Site%20Document%20Library/Home-Fire-Prevention-and-Preparedness.pdf Accessed May 7, 2008. (Link Updated 5/13/2015)
INVESTIGATOR INFORMATION
This investigation was conducted by CDR Steve Berardinelli and Stacy C.Wertman, Safety and Occupational Health Specialists with the Fire Fighter Fatality Investigation and Prevention Program, Fatality Investigations Team, Surveillance and Field Investigations Branch, Division of Safety Research, NIOSH located in Morgantown, WV. Paul Moore, Chief of the Fatality Investigations Team, assisted in this investigation. A technical review was provided by Deputy Chief William Goldfeder, Loveland-Symmes Fire Department (Ohio). The analysis of the bunker gear was conducted by Jeff Stull, International Personnel Protection, Inc.
PHOTOS AND DIAGRAMS
 |
 |
 |
 |
 |
 |
This page was last updated on 11/28/08.