
Laborer Crushed Under Overturned Road Milling Machine
New Jersey Case Report: 03NJ086
Report Date: November 29, 2004
Summary
On September 30, 2003, a 24-year-old construction laborer was killed when he was crushed under an overturning road milling machine. The incident occurred at the construction site of a new taxiway at a large international airport. The construction company was using a large, diesel-powered milling machine (profiler-reclaimer) to remove an old concrete taxiway before building the new taxiway. This tracked machine used a rotating milling drum to remove a 12’ wide strip of pavement to a predetermined depth. The machine is guided forward by the operator as two groundsmen walk along each side of the machine to monitor and adjust the cutting depth. At the time of the incident, the machine operator had finished milling a section of pavement and was backing the machine into position to mill the next section. As the operator moved the machine into place, the tracks went up onto an elevated section of pavement, rocks, and debris. This caused the machine to tip sideways too quickly to allow the operator to compensate with the machine’s controls, and the machine rolled over onto its side. Unknown to the operator, the victim, who was acting as a groundsman, was along side of the machine as it rolled over. He was crushed and killed instantly under the machine. The operator and second groundsman were not injured in the incident. NJ FACE investigators recommend following these safety guidelines to prevent similar incidents:
- Machine operators must be trained to ensure that equipment is operated within the manufacturer’s design specifications.
- Employers must ensure that machinery is operated in accordance with manufacturer’s directions.
- Milling machine manufacturers should install active warning devices to alert the operators when the machine’s slope limitations are being approached.
Introduction
On October 1, 2003, a federal OSHA compliance officer notified NJ FACE Program staff of a laborer killed in a machine-related incident at an airport construction site. A FACE investigator subsequently arranged to observe the OSHA interviews with the company workers on October 10, 2003. The FACE investigator returned on October 28 for a private interview with the owner of the company. Due to the complexity of the equipment, NJ FACE staff requested technical assistance from the NIOSH FACE Program staff. On November 11, 2003, NIOSH safety engineers, OSHA compliance officers, and NJ FACE investigators met to examine the milling machine, which had been transported to a service facility for repair and resale. During the visit, investigators spoke with the service personnel, and examined and photographed the machine. On December 19, 2003, a FACE investigator and OSHA compliance officer met to interview the Airport Police investigator in charge of the incident investigation. The Police investigator provided extensive information from their investigation, including aerial photographs, global positioning system data, and written reports. The incident site (with the construction completed) was briefly viewed and photographed. Additional information for this report was obtained from the NIOSH safety engineers, OSHA investigation file, and the Medical Examiner’s report.
The victim’s employer was a construction contractor specializing in heavy roadway and asphalt paving (SIC 1611, NAICS 237310), as well as utility and other related work. Founded in 1968, the company employed approximately 135 union and office workers at the time of the incident. The company had a comprehensive health and safety program, which included a written safety program, a health and safety committee, and on-site “toolbox” safety meetings. A safety consultant was retained by the company and was present during the employee interviews. Employees were hired from the local union hall when needed and went through a 30-day trial period. Job training was primarily on-the-job supplemented with instruction and manuals. The company had an active labor union.
The victim was a 24-year-old white male construction worker who had worked for the company for the past five years. The victim’s father was a long-time company employee and helped him obtain a job with the company when he was 19 years old. The company owner was a family friend of the victim and his father, and had known the victim since he was 10 years old. The victim was a union member, and had received safety training from the company and on-the-job training from his foreman.
Back to Top
Investigation
Background
The incident occurred at a large international airport in an urban area. The 2,027-acre airport was undergoing a 3.8 billion dollar development program that included extending the train system, modernizing terminals, and expanding and improving the airport’s network of roadways, runways, and taxiways. The airport maintains twelve miles of 75-foot-wide taxiways that connect the airport’s three runways with the central terminal and cargo areas. The victim’s company had been subcontracted to remove and rebuild sections of the airport taxiways. Work on the site started in September, 2002.
The airport taxiways were constructed of concrete atop a base of LCF (lime, concrete, and fly ash), a low-strength concrete. These layers were built on a subsurface of compacted bog sand, which had been trucked in from the NJ shore as landfill when this section of the airport was built in the early 1970’s. The company was using a milling machine (technically known as a profiler/reclaimer) to remove the old taxiways. This large, diesel-powered machine directed a rotating drum set with carbide-tipped steel bits against the road surface to dig it up, and were designed to cut at exact, specified depths and slopes. The subcontractor owned and maintained the milling machines, which were reportedly in good operating condition.
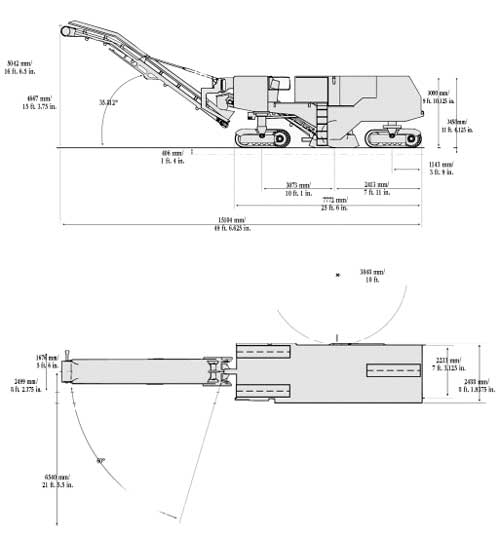
The machine involved in the incident had a specified weight of 80,760 pounds and was equipped with an 800 horsepower diesel engine. The manufacturer listed its operating dimensions as 10’ wide, 9’ 10” high, and 49’ 6” long (see Figure 1). This machine ran on three caterpillar tracks, with two tracks in the front and a single, central track in the rear. All three tracks had listed measurements of 7’ 9” long and were mounted on steering pivots. The front tracks were 14” wide, and the rear track was 18” wide. The machine could travel at an operating (milling) speed of up to 308 feet per minute and a traveling speed of up to 3.5 miles per hour. A 1,300-gallon water tank supplied water to the spray nozzles for the 176 bits on the cutting drum. The machine’s standard cutting width was 7 feet with a maximum cutting depth of 12 inches. Cutting tolerances were specified to be within three millimeters.
|
|
Figure 1. Manufacturer’s illustration of profiler/reclaimer.
|
To operate the milling machine, the operator stood at a control station located toward the front of the machine, about six feet off the ground. The design of the control station provided the operator with easy physical access to either side of the machine. The machine was positioned with the two front tracks forward, and a dump truck was positioned under the built-in conveyor to collect the milled material (see Photo 1). The cutting depth was set by adjusting the height of the tracks, each of which could be independently raised and lowered. This lifted the body of the machine off the ground, which set the height of the fixed cutting drum, located in the center of the machine. This feature allowed the machine to operate on uneven road surfaces, as one track could be set higher than the other to keep the cutting drum level. The cutting depth was maintained with an elevation sensor on each side of the machine. The sensor resembled a small outrigger, which swung away from the machine. Each sensor had a small wheel that followed the road surface and allowed the machine to correct itself. The sensors could be set to operate automatically, or in manual mode with a worker walking beside it to make the adjustments. Once set up, the operator moved the machine forward, causing the rotating cutting drum to mill and remove the road surface. Once the removal of a section (usually a long strip) was completed, the operator would back the machine to the starting point, position it for the next section, and resume milling.

|
|
Photo 1. Manufacturer’s photo of machine in use.
|
The operator’s station had a bubble level to indicate the side slope (lateral incline) of the machine. This level was located on a bulkhead forward of the operator’s control panel, out of sight from the main controls. The bubble level was “red tagged” at its extreme ranges of 15% (the manufacturer’s maximum specification to prevent tipping the machine). The machine did not have any type of tip-over warning device.
Incident
The incident occurred on Tuesday, September 30, 2003, at 12:07 p.m. The weather that day was sunny and clear with temperatures in the mid-60s. Work had started early that morning at another site, a bridge deck project on a major highway. This type of highway work was often done at night or the early morning to prevent disrupting rush-hour traffic. The crew met at 5:00 a.m. and started milling the bridge deck at 5:30 a.m., working for a few hours until traffic increased. They then moved to the airport worksite, arriving there at approximately 9:00 a.m. The crew started work about 30 minutes later and planned to work until their usual quitting time of 1:00 to 2:00 p.m.
The milling crew consisted of the milling machine operator and two groundsmen. Other people working in the immediate vicinity included dump truck operators who collected and carried away the milling waste, and company supervisors who traveled around the construction site. Before starting work, the operator conducted a visual inspection of the machine to check the grease and oil levels, and found everything to be normal. The section to be milled was a straight run of taxiway that had been marked out in advance. The area had been previously milled to remove the concrete surface, leaving an average of about five inches of LCF to be removed. Since the thickness of the LCF varied, the two groundsmen were assigned to walk on each side of the machine to manually adjust the cutting depth as the machine moved forward. A dump truck was positioned under the conveyor to catch the milling debris, with another truck nearby to take its place when the first was full. The crew started work, with the victim walking along the side of the machine as a groundsman. The victim’s foreman was acting as the second groundsman, walking along the opposite side of the machine.
The crew worked through the morning without any reported problems. Shortly before noon, they stopped work so a water truck could refill the milling machine’s water tank. They were also waiting for the dump trucks, which were away unloading the milling waste. The operator started backing the milling machine into position to remove the next section of LCF, with the foreman/groundsman acting as a spotter to help guide the operator. The operator set one of the front tracks on the higher LCF surface and the second track on the lower sand subsurface. The rear steering track was also on the LCF. The LCF in this area was thicker than usual, and there were small mounds of concrete debris in the area. As the machine backed over one of these mounds, the difference between the lower and higher tracks exceeded the machine’s slope design limitations. The operator said that he felt the machine “kick” and start to tip, and tried to level out the machine by adjusting the track height. The foreman/groundsman yelled for him to “watch out!,” and the operator held on to the machine and jumped off as it rolled over on its side. The victim was walking to the left of the machine when it rolled over onto him. Both the operator and the foreman/groundsman went to help, and found him trapped under the machine with water from the water tank pouring on him. A worker crawled under the machine and lifted the victim’s head away from the pooling water, while the airport police and rescue team responded immediately. An excavator was used to lift the machine off the victim, and resuscitation efforts were started. The victim was pronounced dead at 12:35 p.m. by telemetry while enroute to the hospital.

|
|
Photo 2. Photo of incident site showing excavator lifting machine. (Port Authority Police)
|
This incident was thoroughly investigated by the Port Authority Police of NY & NJ, who have jurisdiction over the airports in the area. Their investigation was supplemented with aerial photography, the use of a global positioning system (GPS) to computer-map the incident area, and soil density tests of the sand subsurface. Some of their observations and conclusions included:
- The GPS computer mapping determined that the slope of the milling machine when it tipped was 20.73%, or 11.67 degrees. This was determined by taking measurements at the highest point (a mound of debris) and the lowest point (sand) the machine was on before it went over. The police concluded that the machine exceeded the manufacturer’s design specifications by 5.73%, or 3.17 degrees.
- Soil density tests indicated that the sand could support the milling machine on three tracks. The machine had one track on the sand prior to the incident. During the incident, the tipping machine put most of it’s weight on this track, which the sand could not support. This further increased the slope as the sand compressed and gave way beneath the track.
Back to Top
Recommendations/Discussion
Recommendation #1: Machine operators should be trained to ensure that equipment is operated within the manufacturers design specifications.
Discussion: This incident occurred when the milling machine was backed up onto an uneven surface, placing the machine on a slope greater than it was designed for. To prevent further incidents, NJ FACE recommends that machine operators receive training and periodic retraining that includes the design limits of the equipment. Similar training should also be given to the groundsman so they know the machine’s limits while acting as spotters for the operator.
Recommendation #2: Employers should ensure that machinery is operated in accordance with manufacturers directions.
Discussion: During the examination of the machine, damage was noted that indicated that the cutting drum was rotating at the time of the incident (see Photo 3) when the machine was reportedly being backed into position. The operator’s manual states that the cutting drum should not be engaged until a number of steps are completed, including adjusting the conveyor and elevation sensors. The manual also clearly warns that: · Lowering the cutter too quickly when starting a cut will cause the machine to ride up onto the cutter and lunge backward.
- If the cutter hits an obstruction, the machine may lunge backward.
- Either of these can cause personal injury.
- Lower the cutter slowly. Keep all personnel at least 25 feet away from the rear of the machine while it is in operation.
It is possible that the kick felt by the operator before the machine tipped was the rotating cutter contacting the uneven surface and/or debris. It is not known if this directly contributed to the incident, however the above warnings indicate that this could cause the machine to move backward uncontrollably.

|
|
Photo 3. Damage caused by rotating drum bearing cutting through machine’s sheet metal during tip-over.
|
Recommendation #3: Milling machine manufacturers should install active warning devices to alert the operators when the machine’s slope limitations are being approached.
Discussion: This machine was not equipped with any devices to warn the operator of an impending tip-over situation. Although it did have a bubble level for indicating the approximate slope of the machine, this indicator was not easily seen from the operator’s station. To prevent further tip-overs, NJ FACE recommends that milling machine manufacturers install a visual and audible warning device that activates when the machine approaches its slope limitations. This may provide enough warning for the operator to correct a problem before a tip-over occurs.
A more sophisticated device could be considered which would link the warning device with a microprocessor that could control the machine’s hydraulic system. Such a device could sense a danger situation and automatically adjust the track height to keep the machine from tipping over. This device would have the advantage of having faster reaction time than an operator trying to make manual adjustments.
Recommended Resources
It is extremely important that employers obtain accurate information on health, safety, and applicable OSHA standards. NJ FACE recommends the following sources of information which should help both employers and employees:
U.S. Department of Labor, Occupational Safety & Health Administration (OSHA)
Federal OSHA will provide information on safety and health standards on request. OSHA has several offices in New Jersey that cover the following counties:
Hunterdon, Middlesex, Somerset, Union, and Warren counties
Telephone: (732) 750-3270
Essex, Hudson, Morris, and Sussex counties
Telephone: (973) 263-1003
Bergen and Passaic counties
Telephone: (201) 288-1700
Atlantic, Burlington, Cape May, Camden, Cumberland, Gloucester, Mercer, Monmouth, Ocean, and Salem counties
Telephone: (856) 757-5181
Federal OSHA
Web site: https://www.osha.gov/external icon
U.S. Department of Labor, Mine Safety & Health Administration (MSHA)
Federal MSHA regulates safety and health in metal and non-metal mines. The MSHA website has a great deal of useful safety and health information including detailed reports on fatality investigations. New Jersey mines are under the jurisdiction of the Wyomissing, PA field office.
Telephone: (610) 372-2761
Web site: http://www.msha.govexternal icon
NJ Public Employees Occupational Safety and Health (PEOSH) Program
The PEOSH act covers all NJ state, county, and municipal employees. Two state departments administer the act; the NJ Department of Labor and Workforce Development (NJDLWD), which investigates safety hazards, and the NJ Department of Health and Senior Services (NJDHSS) which investigates health hazards. PEOSH has information that may benefit private employers.
NJDLWD, Office of Public Employees Safety
Telephone: (609) 633-3896
Web site: http://lwd.dol.state.nj.us/lsse/employer/Public_Employees_OSH.htmlexternal icon (Link updated 3/26/2013)
NJDHSS, Public Employees Occupational Safety & Health Program
Telephone: (609) 984-1863
Web site: http://www.state.nj.us/health/eoh/peoshwebexternal icon
NJDLWD Occupational Safety and Health On-Site Consultation Program
Located in the NJ Department of Labor and Workforce Development, this program provides free advice to private businesses on improving safety and health in the workplace and complying with OSHA standards.
Telephone: (609) 984-0785
Web site: http://lwd.dol.state.nj.us/labor/lsse/employer/Occupational_Safety_
and_Health_Onsite_Consultation_Program.htmlexternal icon (Link updated 4/1/2009)
New Jersey State Safety Council
The NJ State Safety Council provides a variety of courses on work-related safety. There is a charge for the seminars.
Telephone: (908) 272-7712.
Web site: http://www.njsafety.orgexternal icon
Internet Resources
Other useful internet sites for occupational safety and health information:
https://www.cdc.gov/niosh – The CDC/NIOSH Web site
http://www.dol.gov/elaws/external icon – USDOL Employment Laws Assistance for Workers and Small Businesses.
http://www.nsc.org/Pages/Home.aspxexternal icon – National Safety Council. (Link updated 11/17/2009)
http://www.state.nj.us/health/eoh/survweb/face.htmexternal icon – NJDHSS FACE reports.
References
- Job Hazard Analysis. US Department of Labor Publication # OSHA-3071, 1998 (revised). USDOL, OSHA/OICA Publications, PO Box 37535, Washington DC 20013-7535.
New Jersey FACE Program
Fatality Assessment and Control Evaluation (FACE) Project
Investigation # 03-NJ-086
Staff members of the New Jersey Department of Health and Senior Services, Occupational Health Service, perform FACE investigations when there is a report of a targeted work-related fatal injury. The goal of FACE is to prevent fatal work injuries by studying the work environment, the worker, the task and tools the worker was using, the energy exchange resulting in the fatal injury, and the role of management in controlling how these factors interact. FACE gathers information from multiple sources that may include interviews of employers, workers, and other investigators; examination of the fatality site and related equipment; and reviewing OSHA, police, and medical examiner reports, employer safety procedures, and training plans. The FACE program does not determine fault or place blame on employers or individual workers. Findings are summarized in narrative investigation reports that include recommendations for preventing similar events. All names and other identifiers are removed from FACE reports and other data to protect the confidentiality of those who participate in the program.
NIOSH-funded state-based FACE Programs include: Alaska, California, Iowa, Kentucky, Massachusetts, Michigan, Minnesota, Nebraska, New Jersey, New York, Oklahoma, Oregon, Washington, West Virginia, and Wisconsin.
This NJ FACE report is supported by Cooperative Agreement # 1 U60 OH0345-01 from the Centers for Disease Control and Prevention (CDC). Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the CDC.
To contact New Jersey State FACE program personnel regarding State-based FACE reports, please use information listed on the Contact Sheet on the NIOSH FACE web site. Please contact In-house FACE program personnel regarding In-house FACE reports and to gain assistance when State-FACE program personnel cannot be reached.
