 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
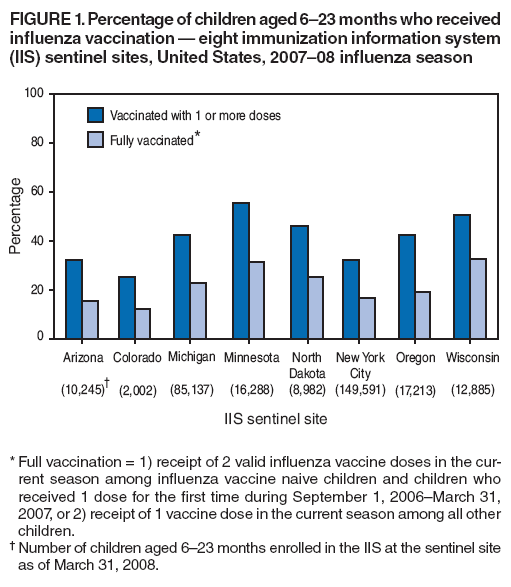
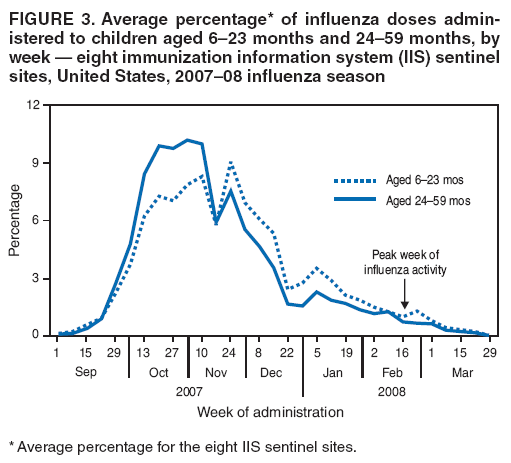
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Influenza Vaccination Coverage Among Children Aged 6--59 Months --- Eight Immunization Information System Sentinel Sites, United States, 2007--08 Influenza SeasonVaccination is the most effective way to prevent influenza-associated morbidity and mortality (1). However, influenza vaccination coverage among children historically has been low (2,3). The Advisory Committee on Immunization Practices (ACIP) recommends annual vaccination with influenza vaccine for all children aged 6--59 months (4). Previously unvaccinated children and children who received only 1 vaccine dose for the first time in the previous influenza season are recommended to receive 2 influenza vaccine doses (4). To assess vaccination coverage among children aged 6--59 months during the 2007--08 influenza season, CDC analyzed data from the eight immunization information system (IIS) sentinel sites.* For the eight sites, an average (unweighted) of 40.8% of children aged 6--23 months received 1 or more influenza vaccine doses, and an average of 22.1% were fully vaccinated. Among children aged 24--59 months, an average of 22.2% received 1 or more doses, and an average of 16.5% were fully vaccinated. These results indicate that influenza vaccination coverage among children remains low (2,3) and highlight the need to identify additional barriers to influenza vaccination and to develop more effective interventions to promote vaccination of children aged 6--59 months who are at high risk for influenza-related morbidity and mortality (1). IISs are useful sources to assess influenza vaccination coverage because data 1) reflect the most recent influenza season, 2) are provider-verified, and 3) can track vaccination patterns throughout the entire influenza season (September--March). For the 2008--2012 Sentinel Site Project period, CDC awarded supplemental funds to eight IISs that met the following criteria: 1) >75% of child vaccine provider sites were enrolled in the IIS, 2) >85% of children aged <6 years who resided in the sentinel site region had two or more vaccinations recorded in the IIS, and 3) >70% of doses administered were reported to the IIS within 30 days of vaccine administration. Sentinel sites in Arizona, Colorado, Michigan, Minnesota, Oregon, and Wisconsin consisted of contiguous geographic counties, postal codes, or census tracts; the other two sentinel sites consisted of the entire state of North Dakota and all New York City boroughs. As of March 31, 2008, the sum of the number of children aged 6--23 months and 24--59 months who were enrolled in the IIS at the sentinel sites ranged from 7,476 in Colorado to 535,877 in New York City. To reflect ACIP recommendations in the 2007--08 influenza season (4), full vaccination was defined as 1) receipt of 2 valid influenza vaccine doses in the current season among influenza vaccine naive children and children who received 1 dose for the first time during September 1, 2006--March 31, 2007, or 2) receipt of 1 vaccine dose in the current season among all other children (4). This definition of full vaccination represented a change from previous influenza seasons, in which children who received only 1 dose in their first year of vaccination were recommended to receive 1 dose in the subsequent season (4). In accordance with ACIP recommendations, doses were considered valid if they were separated by at least 4 weeks. The numbers of children aged 6--23 months or 24--59 months who resided in the sentinel site area and were enrolled in the IIS were the denominators for calculating vaccination coverage at each of the eight sites. The average for the eight sites was calculated by summing the percentages of children vaccinated at each sentinel site and dividing by the total number of sites (eight). Analyses included only children aged 6--23 months or 24--59 months during the entire influenza season to ensure that all children in the study had the same opportunity for vaccination. To determine the weekly pattern of vaccination, at each of the eight sites the number of weekly influenza vaccine doses administered to children aged 6--59 months during the 2007--08 influenza season was determined and converted into a percentage of all doses administered during the entire season; then those eight percentages were averaged. During the 2007--08 influenza season, the average coverage with one or more vaccine doses among children aged 6--23 months was 40.8% (range among the eight sites: 25.2%--55.6%); 22.1% (range: 12.4%--32.8%) were fully vaccinated (Figure 1). Among children aged 24--59 months, the average coverage was 22.2% (range: 11.6%--33.9%) for 1 or more vaccine doses; 16.5% (range: 6.6%--27.2%) were fully vaccinated (Figure 2). Three of the eight sentinel sites (Arizona, Michigan, and Oregon) had reported vaccination coverage data for previous influenza seasons. Minor modifications had been made to these sentinel site geographic areas from the 2006--07 season to the 2007--08 season, making direct comparisons difficult. However, at each of the three sites, the percentage of children receiving 1 or more doses did not change substantially for children aged 6--23 months: Arizona, from 30.4% in 2006--07 to 32.2% in 2007--08; Michigan, from 38.8% to 42.1%; and Oregon, from 46.6% to 42.4%. Coverage with 1 or more doses also did not change substantially for children aged 24--59 months: Arizona, from 15.7% to 14.5%; Michigan, from 19.3% to 21.9%; and Oregon, from 22.4% to 22.8% (2). The average percentage of influenza vaccine doses administered to children aged 6--23 months and 24--59 months across the eight sites increased steadily during September 17--November 16, 2007 (Figure 3). Vaccination declined slightly the week of the Thanksgiving holiday (November 17--23) but rebounded during November 24--30. Among children aged 6--23 months and 24--59 months, <18% and <13% of doses, respectively, were administered during January--March 2008. By week, the greatest average percentages (8.8%--9.1%) of children aged 6--23 months who were partially vaccinated (i.e., required 2 doses but received only 1 dose) received their only dose during November 3--16 or November 24--30. The greatest average weekly percentages (9.2%--10.6%) of partially vaccinated children aged 24--59 months received their single dose during October 20--November 16. Reported by: LJ Williams, MPH, AE Fiore, MD, National Center for Immunization and Respiratory Diseases, CDC; KE White, MPH, Minnesota Dept of Health for the Immunization Information Systems Sentinel Site Project. Editorial Note:These data from the eight sentinel sites reflect the first report of vaccination coverage among children during the 2007--08 influenza season. Four influenza seasons after ACIP recommended annual vaccination for children aged 6--23 months, vaccination coverage in this age group remains low. Coverage at these eight sites was even lower among children aged 24--59 months, two influenza seasons after the ACIP recommended annual vaccination for that age group. Among the three sentinel sites that reported influenza vaccination coverage in previous seasons, no substantial increase in vaccination coverage was observed for the 2007--08 season (2). Administration of influenza vaccine is subject to several challenges that might contribute to low vaccination coverage, including the need to vaccinate each year, the short time period in which to deliver vaccine, limited awareness of the magnitude of influenza burden in young children (5), and the need for 2 doses in the first or second year of vaccination to effectively prevent influenza-related illnesses (6,7). Additional effective educational and programmatic interventions that address these barriers, and studies that identify other barriers to influenza vaccination among parents and vaccine providers, are needed. ACIP recommends that health-care providers offer influenza vaccination to all eligible children who visit for other reasons during the entire influenza season (1). More visits to vaccine providers are required for children aged 6--23 months to meet ACIP vaccination recommendations, compared with children aged 24--59 months; the higher influenza vaccination coverage in the younger age group might have been influenced by more frequent visits to vaccine providers for other reasons. Boosting influenza vaccination coverage will require more parents to be aware of, and act on, the need to schedule visits to providers specifically for influenza vaccination. Emphasizing the benefits of vaccination throughout the influenza season, including in December and beyond, has been advocated as a way to help improve vaccination coverage (1). Campaigns such as National Influenza Vaccination Week† aim to raise awareness about the need for influenza vaccination and to increase vaccination use later in the season. At the IIS sentinel sites during the 2007--08 influenza season, limited vaccination was observed in December and later months. Additionally, across the eight sites, at least 60% of partially vaccinated children aged 6--23 months and 24--59 months received their only dose of vaccine before December, indicating that sufficient time remained to administer the second dose before the end of the influenza season. Vaccine providers and immunization programs can support parent awareness by sending reminder notices. Continued efforts to encourage providers to offer influenza vaccine and to encourage parents to seek vaccination, throughout the influenza season are needed (1). The findings in this report are subject to at least two limitations. First, although the IIS sentinel sites have >75% vaccine provider site participation, not all provider sites in all sentinel sites are enrolled in the IIS. Lacking information on vaccines administered by nonenrolled traditional health-care providers and nontraditional providers (e.g., pharmacists) might have resulted in underestimates of vaccination coverage. Second, these results might not be generalizable to the entire U.S. population and should be viewed as representative of their specific geographic areas only. Protecting young children against influenza and its complications is an important public health goal. Implementation of provider-based strategies shown to be effective in increasing childhood coverage with other vaccines (e.g., reminder notices and extended clinic hours) (8) are particularly important for influenza vaccination, given the limited period during which vaccination occurs. However, specific parent-based and provider-based strategies that address the challenges associated with influenza vaccination also need to be identified, especially as vaccination recommendations expand to include all children aged >6 months during the 2008--09 influenza season (1). Children and adolescents at greater risk for influenza complications, including those aged 6--59 months, should continue to be a focus of vaccination efforts as providers and programs transition to routine influenza vaccination of youths aged >6 months (1). Acknowledgments The findings in this report are based on contributions provided by staff members at eight IIS sentinel sites. References
* An IIS is a confidential, population-based, computerized data system designed primarily to consolidate vaccination records for all children within a geographic area from multiple vaccine providers. Data are collected from health-care providers, vital records, and billing systems. Information regarding IIS sentinel sites is available at http://www.cdc.gov/vaccines/programs/iis/activities/sentinel-sites.htm. † Information available at http://www.cdc.gov/flu/nivw/index.htm.
Figure 1
All MMWR HTML versions of articles are electronic conversions from typeset documents. This conversion might result in character translation or format errors in the HTML version. Users are referred to the electronic PDF version (http://www.cdc.gov/mmwr) and/or the original MMWR paper copy for printable versions of official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Date last reviewed: 9/25/2008 |
|||||||||
|