Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail.
Tiered Use of Inactivated Influenza Vaccine in the Event of a
Vaccine Shortage
The United States has experienced disruptions in the manufacture or distribution of inactivated influenza vaccine
during three of the last five influenza seasons
(1--3). Delays in delivery of influenza vaccine or vaccine shortages remain possible,
in part, because of inherent time constraints in manufacturing the vaccine, given the annual updating of influenza vaccine strains and uncertainties regarding vaccine supply (including licensure of new vaccine preparations). Although total vaccine supply for the 2005--06 influenza season is not yet known, the minimum anticipated supply is approximately 58--60 million doses of inactivated vaccine and 3 million doses of live, attenuated vaccine. This estimated supply is similar to that available during the 2004--05 season and would be adequate to satisfy historical demand for influenza vaccine among persons considered by
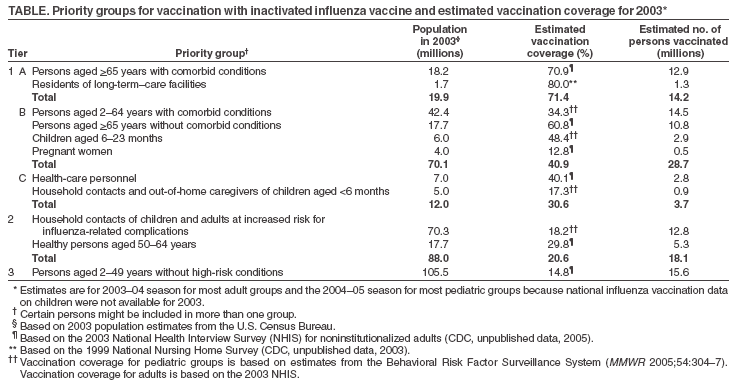
the Advisory Committee on Immunization Practices (ACIP) to be at high risk for serious complications associated with
influenza virus infection, health-care workers, and household contacts of children aged <6 months (Table). These groups
were prioritized for influenza vaccination in 2004--05
(3). Additional doses of inactivated influenza vaccine might be available
for the U.S. market in 2005--06, but this cannot yet be confirmed. Availability of additional vaccine would allow for expansion of the priority groups and, preferably, vaccination of all persons who desire it.
During periods of inactivated influenza vaccine shortfall, vaccination is prioritized on the basis of risk for serious
influenza-associated complications. CDC and ACIP recommend use of vaccination priority groups only in the event of vaccine supply disruptions. At present, CDC and ACIP do not recommend prioritization of inactivated influenza vaccine for the 2005--06 season. Current recommendations for use of influenza vaccine were published recently
(4). However, to help vaccine providers develop contingency plans for the upcoming influenza season in the event of a shortfall, this report details the priority groups for vaccination (Table). Announcement of a need for prioritization will be made promptly upon receipt of
information indicating a potential disruption to the vaccine supply, if necessary.
ACIP and CDC determined the priority groups, ranked in three tiers, on the basis of influenza-associated mortality
and hospitalization rates (Table). In the event of an influenza vaccine shortfall, persons in tier 1 should be vaccinated
preferentially, followed by persons in tier 2, then persons in tier 3. On rare occasions when local vaccine supply is extremely limited, state and local health officials and vaccination providers should prioritize persons in group 1A before all other groups. However,
in all other vaccine shortfall situations, persons in groups 1A, 1B, and 1C should be considered equivalent and should
be vaccinated simultaneously. Eligible persons in group 1C and tiers 2 and 3 should be encouraged to receive live,
attenuated influenza vaccine during periods of inactivated influenza vaccine shortfall.
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services.References to non-CDC sites on the Internet are
provided as a service to MMWR readers and do not constitute or imply
endorsement of these organizations or their programs by CDC or the U.S.
Department of Health and Human Services. CDC is not responsible for the content
of pages found at these sites. URL addresses listed in MMWR were current as of
the date of publication.
Disclaimer
All MMWR HTML versions of articles are electronic conversions from ASCII text
into HTML. This conversion may have resulted in character translation or format errors in the HTML version.
Users should not rely on this HTML document, but are referred to the electronic PDF version and/or
the original MMWR paper copy for the official text, figures, and tables.
An original paper copy of this issue can be obtained from the Superintendent of Documents,
U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800.
Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to
mmwrq@cdc.gov.