|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
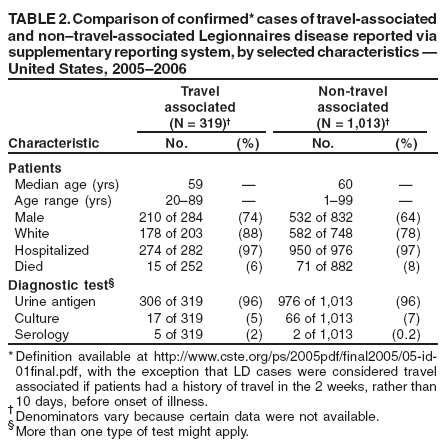
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Surveillance for Travel-Associated Legionnaires Disease --- United States, 2005--2006An estimated 8,000--18,000 persons are hospitalized with Legionnaires disease (LD) each year in the United States (1), and approximately 20% of reported LD cases are associated with travel (2). Outbreaks of travel-associated LD can be difficult to detect because travelers disperse and Legionella-specific diagnostic tests are underutilized (3). Consequently, clinicians and health departments often are unaware when more than one LD case is associated with a common travel destination. In 2005, the Council of State and Territorial Epidemiologists (CSTE) adopted a position statement recommending enhanced surveillance measures for LD, with emphasis on diagnosis and reporting of confirmed travel-associated LD cases within 7 days.* The rationale for enhanced surveillance was that earlier detection might lead to more rapid identification of a source (e.g., cooling tower) and expedite prevention measures (e.g., cleaning and chlorination). To 1) assess data from 32 states that used a supplementary reporting system for LD, 2) describe the epidemiology of travel-associated LD, and 3) compare characteristics of travel-associated cases with those of cases not associated with travel, CDC analyzed LD cases reported via the supplementary system during 2005--2006. The results of that analysis indicated that the proportion of LD cases that were travel associated remained stable from 2005 (23%) to 2006 (25%), the proportion of travel-associated cases reported via a dedicated CDC e-mail address increased from 11% to 24%, and the number of reported clusters of travel-associated LD increased from two in 2005 to eight in 2006. These results suggest that, to fully assess the benefits of enhanced LD surveillance, more states will need to adopt the CSTE recommendations. LD cases are reported to CDC through the National Notifiable Diseases Surveillance System (NNDSS); this system collects certain patient demographic information (e.g., age and state of residence) but not travel history. Since 1980, states have had the option of additionally reporting more detailed information voluntarily to CDC through a supplementary LD reporting system, using a paper case-LD report form† that defines confirmed cases of LD and collects information related to diagnostic testing, location of disease acquisition (i.e., community or hospital), and travel. For this analysis, only confirmed LD cases were included. In 2005 and 2006, totals of 2,301 and 2,834 cases of LD, respectively, were reported to NNDSS, of which 603 (26%) and 729 (26%) cases, respectively, also were reported via the supplementary system (4,5). During 2005--2006, LD cases were reported through the supplementary system by 32 states; five states (Ohio, Michigan, New Jersey, New York, and Virginia) submitted the majority (69%) of supplementary reports. A case of LD was considered to be travel associated if the patient reported spending at least one night away from home during the 2 weeks§ before illness onset; possible nosocomial cases were excluded. Changes in data from 2005 to 2006 were determined to be statistically significant at p<0.05 by chi-square test. The proportions of LD cases that were travel associated and reported via the supplementary system were similar in 2005 (136 of 603 [23%]) and 2006 (183 of 729 [25%]). Reporting via the dedicated CDC e-mail address (travellegionella@cdc.gov), which can facilitate timely reporting, increased significantly, from 15 reports (11%) in 2005 to 44 reports (24%) in 2006 (Table 1). The supplementary system recorded two clusters (defined as two or more cases associated with the same potential source during a 12-month period) of travel-associated LD in 2005 and eight clusters in 2006. Of these 10 clusters overall, seven were associated with hotels, and three were associated with cruise ships; each cluster consisted of either two or three cases of LD. The majority of persons with travel-associated LD had traveled to destinations outside their state of residence. During 2005--2006, the median age was 59 years for persons with travel-associated LD and 60 years for non--travel-associated LD (Table 2). Among those with travel-associated LD, 74% were male, and 88% were white. Among the 252 patients with travel-associated LD and known outcome, 15 (6%) died, compared with 71 (8%) of the 882 patients with non--travel-associated LD. Approximately 96% of both travel-associated and non--travel-associated LD cases were diagnosed by urine antigen testing; few were diagnosed by Legionella culture or serology. Reported by: P Smith, MD, Div of Epidemiology, New York State Health Dept. M Moore, MD, N Alexander, MPH, L Hicks, DO, Div of Bacterial Diseases, National Center for Immunization and Respiratory Diseases; R O'Loughlin, PhD, EIS Officer, CDC. Editorial Note:The 2,301 LD cases reported to NNDSS in 2005 and the 2,834 cases reported in 2006 represent only a fraction of the estimated 8,000--18,000 cases of LD that require hospitalization each year in the United States (1), likely because of underdiagnosis and underreporting. The 2005 CSTE position statement recommended that all cases of LD be reported to CDC to enhance recognition of outbreaks and enable earlier implementation of prevention measures. CSTE also set parameters for timely reporting of travel-associated LD cases, recommending that investigating health departments ascertain whether cases are travel associated and report them to CDC within 7 days of notification of a case. CDC encourages states to submit case-report forms for all LD cases; non--travel-associated cases should be reported to CDC within 30 days. Although the CSTE position statement was not adopted until June 2005, increased use of dedicated e-mail for reporting and improved identification of clusters was noted in 2006 for travel-associated LD. The proportion of LD cases diagnosed by culture has declined since introduction of urine antigen testing (2), and tests are performed on only a limited proportion of patients who have indications for urine antigen testing or Legionella culture of respiratory specimens (6). Despite the convenience of urine antigen testing, the availability of a clinical isolate of Legionella improves the likelihood that an environmental source for Legionella can be identified (i.e., by matching the characteristics of clinical and environmental isolates) and remediated (7,8). In addition, CDC recently implemented DNA sequence-based typing to compare individual clinical strains of Legionella among travelers. Strain typing has contributed to identification of clusters of travel-associated LD in Europe (9) and might provide similar benefits in the United States. Therefore, CDC is requesting that state health departments forward to CDC all clinical isolates of Legionella obtained from persons who report that they traveled during the 2--14 days before onset of illness. Details regarding the isolate submission process can be obtained by e-mail (travellegionella@cdc.gov) or by telephone (404-639-0418). The findings in this report are subject to at least five limitations. First, because analysis was limited to 2005--2006 and the CSTE position statement was adopted in 2005, sufficient time might not have elapsed to attribute changes in LD reporting to the CSTE statement. Second, the data presented likely underestimate the number of cases of LD because diagnostic tests for LD are underutilized in the United States. Utilization might increase as more clinicians follow recently updated guidelines for management of community-acquired pneumonia, including LD (10). Third, travel-associated LD cases might be underestimated because not all clinicians obtain a travel history from all patients with community-acquired pneumonia. Fourth, although an increase in reporting by e-mail might suggest more rapid reporting, timeliness of reporting could not be assessed because the dates that reports were received by CDC were not recorded. Finally, although all states are required to report LD to NNDSS, only 26% of these LD cases also were reported via the voluntary supplementary system during 2005--2006. Therefore, the detailed data provided on case-report forms might not be representative of all reported LD cases. Identification of a single case of LD suggests the possibility of an environmental source to which other persons might be exposed. Therefore, timely reporting all cases of travel-associated LD to CDC is important for identifying clusters. CDC encourages state health departments to post information on LD cases associated with travel on the CDC Epidemic Information Exchange (Epi-X) to alert other health officials to review their records for cases of LD associated with travel to the same destination. During 2005--2006, a total of 30 Epi-X postings asked that cases of LD associated with travel to specific locations be reported to CDC or to the investigating state health department. CDC resources for investigating and reporting cases of travel-associated LD are available at http://www.cdc.gov/legionella. CDC also continues to be available for consultation with regard to LD clusters. References
* Available at http://www.cste.org/ps/2005pdf/final2005/05-id-01final.pdf. † Available at http://www.cdc.gov/legionella/files/legionella_case_report.pdf. § The 2005 CSTE position statement was used to define confirmed cases of travel-associated LD, with the following exception: LD cases were considered travel associated if patients had a history of travel in the 2 weeks, rather than 10 days, before onset of illness. Table 1
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Date last reviewed: 12/5/2007 |
|||||||||
|