|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
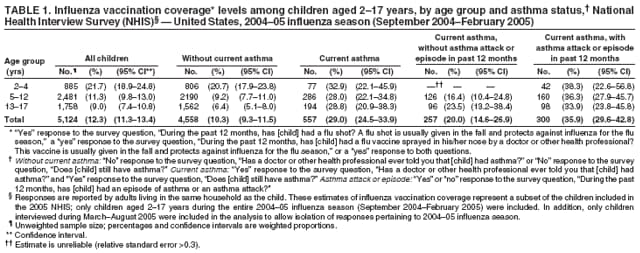
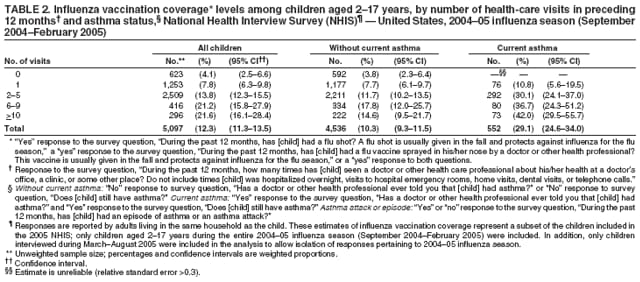
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Influenza Vaccination Coverage Among Children with Asthma --- United States, 2004--05 Influenza SeasonIn 2005, approximately 8.9% (6.5 million) of U.S. children aged <18 years were reported to have current asthma (1). Children with asthma are at high risk for complications from influenza, and influenza vaccination has been determined to safely and effectively reduce rates of influenza in these children (2). Since its establishment in 1964, the Advisory Committee on Immunization Practices (ACIP) has recommended that all children with asthma aged >6 months receive vaccination with inactivated influenza vaccine during each influenza season; however, national influenza vaccination coverage rates specifically for children with asthma have not been determined (2). Previous studies have assessed influenza vaccination rates in children with asthma at the local level using health maintenance organization and clinician group-practice information, with estimates ranging from 10% to 43% for various influenza seasons (3,4). Another study used Behavioral Risk Factor Surveillance System (BRFSS) data to estimate influenza vaccination coverage in children aged 2--17 years with one or more conditions putting them at high risk for complications from influenza (including asthma, although asthma was not assessed separately); in that study, the national rate was estimated at 34.8% for the 2004--05 influenza season (based on a sample size of 685, which included all states and the District of Columbia [DC]) (5). To estimate national influenza vaccination coverage rates among children aged 2--17 years with current asthma,* CDC analyzed data from the 2005 National Health Interview Survey (NHIS). This report describes the results of that analysis and provides the first national estimates of influenza vaccination coverage among children with asthma. The findings indicated that although children with current asthma were more likely to receive influenza vaccination than children without current asthma, the vaccination coverage rate among children with asthma was low, at 29.0% (95% confidence interval [CI] = 24.5--33.9). These findings underscore the need to increase influenza vaccination coverage in children with asthma aged 2--17 years by identifying and overcoming barriers to vaccination. NHIS is an ongoing, cross-sectional, in-person household interview survey of the civilian, noninstitutionalized population of the United States. During the interview, information about one randomly selected child from each family is collected from an adult family member who resides in the same household as the child. The child questionnaire contains several questions that assess asthma status; in 2005, NHIS added questions regarding influenza vaccination for children. Because NHIS interviews are conducted throughout the year, the 2005 questions regarding receipt of influenza vaccination during the 12 months preceding the interview could have elicited responses that referred to vaccination that occurred during the end of the 2003--04 influenza season, the entire 2004--05 season, or the beginning of the 2005--06 season. In addition, participants who were questioned during the 2004--05 influenza season could have reported no influenza vaccination at the time of the survey but then received one later during the same season. To address these methodological concerns and attempt to ensure that the responses included in this analysis were only in reference to the 2004--05 influenza season (September 2004--February 2005), only responses from interviews conducted during March--August 2005 were included in the analysis. Using this methodology, future NHIS data can be analyzed for influenza vaccination coverage by influenza season. In this study, NHIS data from 2005 were used to estimate influenza vaccination coverage during the 2004--05 influenza season for children aged 2--17 years† by asthma status and age group. Coverage also was estimated by asthma status and reported number of visits to a health-care provider in the preceding 12 months. A total of 5,124 children aged 2--17 years were included in the analysis by age group, and 5,097 children were included in the analysis by number of health-care visits. Only children who were aged 2--17 years for the entire 2004--05 influenza season were included. A child was considered vaccinated for the 2004--05 influenza season if the child had a reported date of vaccination during September 2004--February 2005. Of the children in the sample with a reported influenza vaccination in the preceding 12 months, 7.9% were excluded from the analysis for not reporting a date of vaccination. In addition, 7.8% of those with a reported influenza vaccination in the preceding 12 months were not included because their reported date of vaccination did not occur during September 2004--February 2005 (i.e., reported vaccination occurred during months in which the influenza vaccine was likely unavailable). Univariate analysis was performed, and samples were weighted to produce national estimates. Influenza vaccination coverage for the 2004--05 influenza season among children aged 2--17 years was 29.0% for children with current asthma and 10.3% for children without current asthma. Children with current asthma had similar rates of vaccination among all age groups, ranging from 32.9% to 28.0% among children aged 2--4 years and 5--12 years, respectively. In contrast, children without current asthma had a wider variation in vaccination coverage by age group, with younger children having higher rates of vaccination than older children (20.7% for ages 2--4 years versus 6.4% for ages 13--17 years, p<0.001 by t test) (Table 1). Calculation of influenza vaccination-coverage rates in children with current asthma who had experienced an asthma attack or episode during the 12 months preceding the interview indicated that these children had higher coverage rates than those without an attack or episode (35.9% versus 20.0%, p<0.001, by chi-square test). The lowest vaccination rate among children with current asthma (16.4%) was for children aged 5--12 years who had not had an asthma attack or episode in the 12 months preceding the interview. Among children with the same number of health-care visits during the 12 months preceding the interview, children with asthma who had two through five or >10 health-care visits had higher rates of influenza vaccination than children without asthma (Table 2). In addition, influenza vaccination coverage among children with current asthma increased as the reported number of health-care visits increased. Approximately 10.8% of children with current asthma who had one health-care visit in the preceding year were vaccinated, whereas 42.0% of children with current asthma who had >10 visits were vaccinated. Reported by: SN Brim, MA, RA Rudd, MSPH, RH Funk, DVM, DB Callahan, MD, Div of Environmental Hazards and Health Effects, National Center for Environmental Health; GL Euler, DrPH, Immunization Svcs Div, National Center for Immunization and Respiratory Diseases (proposed), CDC. Editorial Note:The findings in this report, based on 2005 NHIS data, include the first national estimate of influenza vaccination coverage in children with current asthma. The analysis indicated a lower coverage rate (29.0%) during the 2004--05 influenza season than a previous study based on BRFSS data (34.8%) that included children with conditions placing them at high risk for influenza complications (5). Because BRFSS and NHIS have different survey methodologies, a difference was not unexpected. The BRFSS analysis included children with conditions other than asthma, including other lung problems, heart problems, diabetes, kidney problems, a weakened immune system, anemia, or aspirin therapy for chronic conditions. In addition, this study based on NHIS data used September--February as its time frame for influenza vaccination, whereas the BRFSS study used September--January. Finally, BRFSS is conducted in all states and DC, whereas NHIS uses a sampling method designed to produce an accurate national estimate without including all states. An unexpected influenza vaccine shortage occurred during the 2004--05 influenza season. In October 2004, within days of the first indication of the shortage, CDC released interim recommendations for prioritizing influenza vaccine distribution. Children aged 2--17 years with asthma were included in the priority group of "persons aged 2--64 years with underlying chronic conditions" (6). This interim recommendation might have contributed to the higher influenza vaccination rates for children with asthma compared with children without asthma as clinicians followed recommendations; alternatively, the shortage might have led to an overall decrease in coverage rates among all children, including children with asthma, compared with rates from other seasons. The results of this analysis cannot be compared with previous years because 2005 was the first year that NHIS included influenza vaccination questions on the child portion of the survey. Analysis of NHIS data from 2006 and future years will allow determination of trends in national influenza vaccination coverage in children with asthma. The differing coverage rates, by age, among children without current asthma likely are a result of various factors. For example, the high rate of vaccination in children aged 2--4 years compared with other ages might be a reflection of the regularly scheduled pediatric well-child visits for young children, which might result in receipt of an influenza vaccination. In addition, physician awareness of the increased risk for influenza complications in children aged 2--4 years might have contributed to this higher vaccination rate. The findings in this report are subject to at least three limitations. First, the results might be affected by recall bias, which might cause underreporting of vaccination directly proportional to the time between vaccination and interview. However, if parents of children with asthma preferentially recall influenza vaccination, this would contribute to higher coverage estimates for children with asthma compared with children without asthma. Second, inaccurate reporting of vaccination dates might cause misclassification of responses during the analysis; NHIS responses for children are based on report by an adult and are not confirmed by health-care providers. Finally, whether children aged <9 years who were receiving their first influenza vaccination also received the second dose recommended by ACIP for maximum protection could not be determined on the basis of NHIS data (2). In February 2006, ACIP expanded its influenza vaccination recommendation to include all children aged 6--59 months, and the committee also is evaluating a universal influenza vaccination strategy (7). Continued monitoring of influenza vaccination coverage among children with asthma in future influenza seasons is needed to determine how these recommendations affect coverage rates in this population. The findings in this analysis indicate that influenza vaccination coverage among children with asthma is inadequate and that opportunities for vaccination during health-care provider visits likely are being missed. Previous studies have assessed methods to improve influenza vaccination rates, such as year-round scheduling of fall and winter influenza vaccination appointments and computerized reminder systems (8,9). In one study, the percentage of children with asthma who received at least 1 dose of influenza vaccine increased from 23.2% to 35.1% (p<0.001) after implementation of a year-round scheduling policy (8). National trends in coverage should be monitored so that public health policies can better target vaccination of all children with asthma, and correlates of vaccination among children with asthma should be explored so that measures can be developed for groups of children with asthma who have the lowest rates of vaccination. Increasing influenza vaccination coverage in this population will help decrease influenza and its associated complications. References
* Current asthma: "Yes" response to the survey question, "Has a doctor or other health professional ever told you that [child] had asthma?" and a "yes" response to the survey question, "Does [child] still have asthma?" Without current asthma: "No" response to the survey question, "Has a doctor or other health professional ever told you that [child] had asthma?" or a "no" response to the survey question, "Does [child] still have asthma?" Asthma attack or episode: "Yes" response to the survey question, "During the past 12 months, has [child] had an episode of asthma or an asthma attack?" † Children aged <2 years were not included because 1) asthma diagnoses are considered unreliable in children at this age, 2) the 2004--05 influenza recommendations called for vaccination of all children aged 6--23 months regardless of asthma status (therefore, ages 2--17 years were the only ages with influenza vaccination recommendations specific to children with asthma), and 3) previous BRFSS studies used an age range of 2--17 years.
Table 1
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Date last reviewed: 3/8/2007 |
|||||||||
|