|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
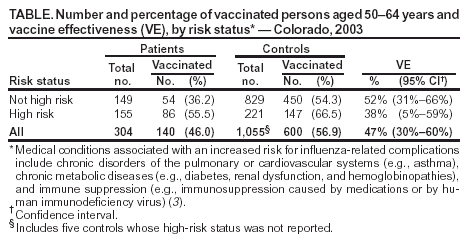
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Assessment of the Effectiveness of the 2003--04 Influenza Vaccine Among Children and Adults --- Colorado, 2003The 2003--04 influenza season was characterized by the early onset of influenza activity, reports of severe illness, particularly in children, and predominant circulation of an influenza A (H3N2) virus strain that was antigenically different from the influenza A (H3N2) vaccine strain (1). In 2003, a retrospective cohort study among children and a case-control study among adults in Colorado were conducted to provide preliminary data on the effectiveness of the 2003--04 influenza vaccine. This report summarizes the results of those studies, which indicated vaccine effectiveness (VE) among both adults and children, differing from results of a previous study that did not indicate effectiveness among adults (2). Retrospective Pediatric Cohort StudyUsing electronic medical records and an immunization registry database from 2003, Kaiser Permanente Colorado and CDC conducted a retrospective cohort study among children aged 6--23 months. The objective of the study was to evaluate the effectiveness of the 2003--04 influenza vaccine against medically attended illnesses that occurred during November 19--December 7, 2003, the period of peak influenza activity in the Denver metropolitan area. Two different outcomes based on International Classification of Diseases, Ninth Revision (ICD-9)-coded health-care provider visits were evaluated: influenza-like illness (ILI) and pneumonia and influenza (P&I)*. Children included in the study were aged 6--23 months on October 1, 2003, were continuously enrolled in the Kaiser Permanente Colorado Health Maintenance Organization (HMO) during October 1--December 31, 2003, and had one or more health-care visits to the HMO since birth or >8 months before October 1, depending on the child's age. Children who had received two influenza vaccinations >14 days before diagnosis of ILI or P&I and who had received at least one of their two influenza vaccinations since September 2003 were classified as fully vaccinated. Children with no influenza vaccination since September 2003 were classified as unvaccinated. Children with 2 doses since September 2003 but who sought medical attention <14 days after their second dose, or children with only 1 dose of influenza vaccine since September 2003 and no previous influenza vaccination, were classified as partially vaccinated. Because patients continued to be vaccinated during the influenza season, vaccination status was included as a time-varying variable by using a multivariate Cox proportional hazard model to estimate a hazard ratio (HR). VE was calculated as one minus HR. Chronic medical conditions†, age, and sex were controlled for in the analysis. A total of 5,139 children were included in the analysis; 2,518 (49%) were female, and 382 (7%) had one or more chronic medical conditions. By November 19, totals of 377 (7%) and 1,007 (20%), respectively, were fully or partially vaccinated against influenza; by December 7, totals of 752 (15%) and 1,388 (27%), respectively, were fully or partially vaccinated. The estimated HRs were 0.75 (95% confidence interval [CI] = 0.56--1.00) for ILI and 0.51 (95% CI = 0.29--0.91) for P&I, when fully vaccinated children were compared with unvaccinated children, and corresponded to VE estimates of 25% (p = 0.052) and 49% (p = 0.022), respectively. When partially vaccinated children were compared with unvaccinated children, no statistically significant reduction in ILI or P&I was observed. Adult Case-Control StudyDuring December 2003--February 2004, a case-control study was conducted among persons aged 50--64 years by CDC and the Colorado Department of Public Health and Environment (CDPHE). Patients were identified from cases of laboratory-confirmed influenza reported to the CDPHE surveillance system during November 1--December 31. Contact information was not routinely included or required with case reports and limited the number of patients who could be contacted. Patients were interviewed by telephone, and information was collected on demographics, illness onset and duration, vaccination and timing, health-care provider visits, hospitalization, and use of antiviral medication. Controls were recruited through random-digit--dialing sampling and were matched 3:1 to patients by age, sex, and telephone area code. During telephone interviews, information on demographics, vaccination and timing, and history of ILI was collected. Logistic regression analysis that controlled for influenza-related high-risk conditions (3), sex, and telephone area code was used to estimate an odds ratio (OR). VE was calculated as one minus OR. Of 574 patients reported to CDPHE, 352 (61%) were contacted; 330 (94%) agreed to participate. Patients were excluded if they did not recall influenza testing or experiencing symptoms of illness or if they were vaccinated 1--13 days before influenza illness onset; 304 cases were included in the analysis. Of 1,675 eligible controls, 1,482 (88%) were contacted; 1,185 (80%) completed the interview. A total of 130 reported having ILI and were excluded; 1,055 controls were included in the analysis. The patients were older (mean age: 57 years among patients and 56 years among controls; p<0.0001), and 166 (50%) had medical conditions placing them at increased risk for influenza-related complications, compared with 221 (21%) of controls (p<0.01) (3). Thirty-two percent of patients were hospitalized during their influenza illness. VE was estimated at 52% for those without a high-risk condition and 38% for those with a high-risk condition (Table). Reported by: D Ritzwoller, PhD, S Shetterly, MS, K Yamasaki, PharmD, E France, MD, Kaiser Permanente Colorado, Denver; K Gershman, MD, A Shupe, PhD, Colorado Dept of Public Health and Environment. J Alexander, MD, F Averhoff, MD, C Bridges, MD, C Brown, MS, S Chaves, MD, M Cortese, MD, G Euler, PhD, P Gargiullo, PhD, G Herrera, MD, M Iwane, PhD, M Kolczak, PhD, J Seward, MBBS, Epidemiology and Surveillance Div, National Immunization Program, CDC. Editorial Note:The findings from the two studies indicated that the influenza vaccine had some effectiveness (25%--49% against nonlaboratory-confirmed influenza and 38%--52% against laboratory-confirmed influenza) in preventing illness during the 2003--04 influenza season, supporting recommendations to continue influenza vaccination efforts despite a suboptimal match between the predominant influenza A (H3N2) circulating and vaccine strains (1,2). The effectiveness of the inactivated influenza vaccine against laboratory-confirmed illness among healthy adults aged <65 years is expected to be 70%--90% in years when the vaccine and circulating strains are well matched (3--5). The estimated 52% VE against laboratory-confirmed influenza among adults with no high-risk conditions in this study was lower, but still provided substantial health benefit. The study among children aged 6--23 months provides further data that 2 doses of vaccine (i.e., a dose of the current vaccine plus a primer dose) are needed to optimize protection compared with a single dose (3). Results from these studies differ from those of a study of health-care workers that did not find the 2003--04 influenza vaccine to be effective against ILI (2). However, the health-care worker study might have had an insufficient number of subjects to detect low effectiveness against ILI compared with the pediatric ILI study, which included approximately three times as many subjects in a population expected to have a higher influenza illness attack rate than adults (3). In addition, the more specific outcome of medically attended, laboratory-confirmed influenza used in the case-control study of persons aged 50--64 years was more likely to find effectiveness, compared with the less influenza-specific ILI outcome used in the health-care worker study (1,4,5). The findings in this report are subject to at least three limitations. First, because both studies in this report were retrospective and vaccination was not assigned randomly, biases in VE estimates might have occurred. However, these estimates are consistent with other studies that evaluated influenza VE in years with and without an antigenic mismatch by using ILI, laboratory-confirmed influenza, and more severe illness outcomes such as P&I hospitalization (3--7). Second, the studies are limited by lack of testing for influenza among the children and among adult controls and lack of validation of influenza vaccination among the adults; however, reporting of influenza vaccination has been found to be sensitive and specific among elderly outpatients (8). Third, adults without telephones in the control group were not eligible to participate; persons living in households without telephones might be less likely to report influenza vaccination, compared with those living in households with telephones (9). Influenza vaccine remains the primary means for the prevention of influenza and its complications and can provide benefit even in years when the influenza vaccine and circulating strains are not matched optimally. Efforts to increase vaccination rates in groups at high risk and their contacts are needed to reduce the burden of influenza. In addition, vaccination with 2 doses of influenza vaccine for children not vaccinated previously against influenza is needed to maximize protection. For optimal assessment of influenza VE, prospective studies should be conducted annually. Acknowledgment The findings in this report are based in part on contributions by D Ferguson, MD, EIS Officer, CDC. References
* For ILI, ICD-9 codes were 38, 78.89, 78.99, 460--464.2, 464.4, 465--466, 480--487, 490, and 780.31; and 493, 786.07, 786.1, and 786.2 plus fever ICD-9 code 780.6 or a measured temperature of >100.4º F (>38.0º C) at health-care visit. For P&I, codes were 480--487. † Medical conditions associated with an increased risk for influenza-related complications include chronic disorders of the pulmonary or cardiovascular systems (e.g., asthma), chronic metabolic diseases (e.g., diabetes, renal dysfunction, and hemoglobinopathies), and immune suppression (e.g., immunosuppression caused by medications or by human immunodeficiency virus) (3).
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 8/12/2004 |
|||||||||
This page last reviewed 8/12/2004
|