|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
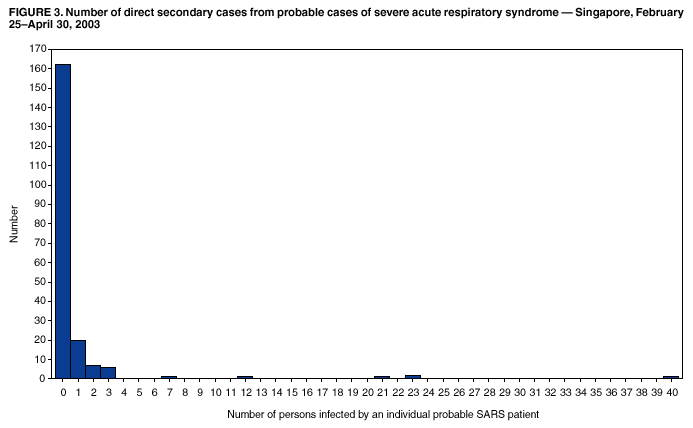
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Severe Acute Respiratory Syndrome --- Singapore, 2003The Singapore Ministry of Health (MOH), with assistance from the World Health Organization (WHO), has been investigating an outbreak of severe acute respiratory syndrome (SARS). This is a novel condition caused by the SARS-associated coronavirus (SARS-CoV) and is characterized by both an atypical pneumonia and efficient nosocomial transmission. This report summarizes epidemiologic features of this outbreak in Singapore, including the influence of super spreaders* and the national prevention and control strategy.† On March 6, 2003, MOH was notified about three persons who had traveled to Hong Kong during late February and were admitted during a 5-day period to local hospitals for pneumonia (1). These patients included Case 1 and a traveling companion. They had been guests at Hotel M (Kowloon, Hong Kong) on February 20 and 21, coinciding with the stay of a person with SARS who transmitted disease to at least 13 guests (2). On March 14, MOH was notified about six persons, including two health-care workers (HCWs), who were admitted to Tan Tock Seng Hospital (TTSH) for atypical pneumonia; all had close contact with Case 1. Since late March, the outbreak has been characterized by nosocomial transmission caused by persons who were not immediately recognized as having SARS. The first major extension of this illness outside the health-care setting was from a recent probable SARS patient to two taxi drivers and the patient's coworkers in a wholesale market. In Singapore, suspect and probable cases are identified and reported by using a modification of the WHO case definition that expands contact to include any health-care setting. Surveillance for suspect cases includes any fever and/or respiratory symptoms among HCWs, clusters of cases of community-acquired pneumonia, unexplained respiratory deaths, and individual cases with no contact but that are clinically suspicious for SARS. An independent, hospital-based surveillance system is being established for community-acquired pneumonia, but the threshold to monitor and investigate any unexplained febrile illness or pneumonia with laboratory testing for SARS-CoV and other etiologies is increasingly low. Source and contact tracing is conducted for probable cases and highly suspicious suspect cases on the basis of epidemiologic and clinical criteria. All persons who were household, social, hospital, and occupational contacts during the 10 days before symptom onset are traced to identify the source of infection; such contacts identified during the period from symptom onset to hospital isolation are traced to identify exposed persons for home quarantine. Summary StatisticsAs of April 30, a total of 201 probable cases of SARS and 722 suspect cases have been reported (Figure 1). The date of isolation of the last autochthonous probable case was April 28. Of the 201 persons with probable SARS, the median age was 36 years (range: 4--90 years; one was aged <12 years); 132 (66%) were female. The probable patients are Singaporean (81%), Filipino (8%), Chinese (5%), Indonesian (3%), Malaysian (2%), and Indian (1%). All persons with probable cases were hospitalized; 143 (71%) have been discharged after a median hospital stay of 11 days (range: 3--46 days). Twenty-two (11%) patients have required mechanical ventilation, and 25 have died (case-fatality proportion: 12.5%). Of the decedents, the median age was 53 years (range: 24--90 years), 14 (56%) were male, and 96% were Singaporean. A total of 26 persons with probable SARS have had virus, viral nucleic acid, or antibody to SARS-CoV detected in body fluids. Of the 84 (42%) HCWs with probable SARS, 49 were nurses; 13, physicians; and 22, persons with other occupations (attendants, radiographers, housekeepers, a porter, and a cleaning supervisor); no SARS cases have been reported among laboratory workers or pathologists. Of the eight travelers who acquired probable SARS outside Singapore, one (Case 1) has resulted in additional cases. For 21 probable cases with well-defined point exposures, the mean incubation period was 5.2 days (±2.5 days) (median: 5 days; range: 1--10 days; 95th percentile = 9 days). For 94 probable cases, the mean incubation period was 5 days (±2.5 days) (median: 4.3 days; 95th percentile = 9.7 days) using the midpoint for well-defined exposures. A total of 172 probable cases are linked through chains of transmission to Case 1 (Figure 2). Two (1%) cases do not have an associated link with another probable case. Twelve (6%) patients have a link to a health-care facility; of these, eight are HCWs, and four are visitors. Of these 12 cases, six might be associated with two inpatients who have yet to be included in the case count; preliminary retrospective investigation suggests that these inpatients have probable cases of SARS. One probable case and seven other probable cases associated with it are linked to the wholesale market cluster. On the basis of surveillance reports, 153 (76%) infections were acquired in a health-care facility; the remainder either have household, multiple, or unknown exposures. Overall, 162 (81%) probable SARS cases had no evidence of transmission to other persons with clinically identifiable illness (Figure 3). Super Spreaders of SARSFive persons with probable SARS cases have been categorized as super spreaders of SARS. These patients appear to have infected > 10 HCWs, family and social contacts, or visitors to the health-care facilities where the patients were hospitalized. Case 1. A person aged 22 years visited Hong Kong for a shopping trip and resided at Hotel M during February 20--25. On February 25, the visitor developed a fever with a dry cough and, on March 1, was hospitalized on Ward 5A of TTSH with a patchy infiltrate on chest radiograph. The patient's platelet count was 105,000/mm3 (normal: 130,000--150,000/mm3); a white blood count was 3,800/mm3 (normal: 4,000/mm3). On March 4, the patient was transferred to the intensive-care unit (ICU) because of decreased blood oxygen saturation. During March 6--11, the patient was admitted to and remained in isolation on Ward 5A. On March 11, the patient was transferred to Ward 8A. This patient was directly linked to probable SARS infection in 21 persons (nine HCWs and 12 family members and visitors) and to suspected SARS in three persons. Of the ill family members and visitors, the patient's mother, father, and a visitor died. SARS-CoV infection in this patient was confirmed by virus isolation, nucleic acid testing, and serology. Case 2. A nurse aged 27 years, who had attended to Case 1 on TTSH Ward 5A, became ill on March 7 and was admitted to Ward 8A on March 10 with fever and sore throat. A white blood count was 2,300/mm3; platelets were 93,000/mm3; and bilateral infiltrates were seen on chest radiograph. The patient had vomiting but no diarrhea. On March 13, the nurse was isolated. This patient is directly linked to probable SARS infection in 23 persons (11 HCWs and 12 family members and visitors) and to suspected SARS in five persons. Case 3. A person aged 53 years with diabetes and ischemic heart disease was admitted on TTSH Ward 8A on March 10 for polymicrobial sepsis with diarrhea. The patient stayed in the same six-person room as Case 2. On March 12, the patient had fever and dyspnea requiring mechanical ventilation and was transferred to the coronary care unit for severe congestive heart failure. On March 20, the patient was isolated. The patient died on March 29. This patient was directly linked to probable SARS infection in 23 persons (18 HCWs and five family members and visitors) and to suspected SARS in 18 persons. Case 4. A person aged 60 years was admitted to TTSH Ward 5A from March 5 to March 20 for chronic kidney disease and diabetes. On March 24, the patient was readmitted to Singapore General Hospital (SGH) Ward 57 for steroid-induced gastritis and gastrointestinal bleeding with melena. The patient had a low-grade fever, and a chest radiograph was normal. On March 28, the patient had high fever (101.8º F [38.8º C]); a repeated chest radiograph remained normal. The patient was treated with antibiotics and, on March 29, was transferred to Ward 58. Tests showed the patient had Escherichia coli bacteremia. On March 30, a chest radiograph was again normal. On April 3, the patient was administered another antibiotic and defervesced. However, on April 4, a chest radiograph showed signs of pneumonia, SARS was considered, and the patient was isolated. A total of 62 persons with probable or suspected SARS (comprising 25 HCWs, 20 inpatients, and 17 family and social contacts) were linked to this case. This patient is linked to 40 patients with probable SARS (37 HCWs and visitors) because of direct contact and might be linked to the remaining probable cases because they traveled the same corridor used by the patient. SARS-CoV infection in this patient was confirmed by nucleic acid testing of a throat swab and stool. Case 5. A vegetable hawker aged 64 years visited Case 4 (the 64-year-old's sibling) in SGH on March 31. The 64-year-old had a history of ischemic heart disease and left ventricular failure. On April 5, the patient had onset of illness with coryza, myalgia, cough, and temperature of 99.9º F (37.7º C). On April 8, the patient was admitted to National University Hospital through the emergency department from his general practitioner's office. The patient had suspected congestive cardiac failure secondary to acute myocardial infarction; the patient had a blood pressure of 80/50 mm and temperature of 95.0º F (35.0º C). The patient was briefly admitted to Ward 64 before being intubated for increased respiratory distress and transferred to the ICU. On April 9, the patient was transferred to TTSH after the history of the patient's visit to SGH was obtained. On April 12, the patient died. This patient is directly linked to infection in 15 persons (five HCWs and two inpatients; two family members; one visitor; two taxi drivers who transported the patient to and from the vegetable stall on April 5 and April 8, respectively; two hawkers in the same wholesale market where the patient worked; and a visitor to the emergency department). Illness in 12 of these persons was consistent with the probable case definition for SARS. SARS-CoV infection in this patient was confirmed by nucleic acid testing of a throat swab and buffy coat sample. In addition to illness caused by these super spreaders, a few smaller clusters of transmission from probable cases have been identified. This includes an eight-person cluster involving a vegetable hawker, his dead wife, and six other family members whose onset dates and links are being verified; a four-person cluster of cases in a long-term--care facility associated with a patient discharged from TTSH on March 23 after 15 days on Ward 7D; and a three-person cluster of secondary cases in National University Hospital initiated by a visitor to TTSH who visited Ward 8A where Cases 2 and 3 were staying. Control MeasuresIn Singapore, infection-control measures have been expanded as the epidemiologic and clinical features that underlie continuing transmission have been recognized. On March 22, TTSH/Communicable Disease Center was designated as the hospital for intake and solitary isolation of all suspect and probable SARS cases. All HCWs attending to patients with suspected or probable SARS are required to wear gloves, gowns, goggles, and N95 or equivalent respirators; positive air purifying respirators (PAPR) are required for high-risk or aerosol-generating procedures. Similar measures have been recommended for HCWs evaluating any person with a febrile illness. By April 9, all staff at SGH were required to adhere to temperature checks for fever twice daily; this initiative has been extended to all HCWs in Singapore. Other measures include stopping hospital visitations, except for pediatric, obstetric, and selected other patients. For these patients, visitors are limited to a single person who must wear a mask and pass a temperature check; all other visits are by videoconference. An audit of infection-control practices is ongoing. On March 24, MOH invoked the Infectious Diseases Act to quarantine all contacts who have been exposed to SARS patients. This legislation allows mandatory home quarantine for 10 days, which is now enforced by CISCO, a Singapore Security Agency. CISCO serves the quarantine order and installs an electronic picture (ePIC) camera at the home of each contact. All inpatients who are discharged from a hospital with previous SARS cases are under telephone surveillance for 21 days; all probable SARS inpatients and selected suspect SARS inpatients who have recovered and are discharged are on home quarantine for 14 days. Patients requiring readmission are admitted only to the same hospital of original admission. A dedicated private ambulance service is sanctioned to transport all suspect or probable cases to the SARS designated hospital, including all febrile persons on home quarantine or from the airport or seaports. On April 20, after the identification of a cluster of illness among employees of a large wholesale market, the market was closed for 15 days and the vendors placed in home quarantine. On April 24, the Infectious Disease Act was amended with penalties for violations 1) to require persons who might have an infectious disease to go to a designated treatment center and to prohibit them from going to public places; 2) to prohibit breaking home quarantine with the possibility of electronic tagging and forced detention for violators; and 3) to permit contaminated areas to be quarantined and any suspected sources of infection to be destroyed. In addition, persons throughout the country have been requested to monitor body temperature and stay home or seek medical care if any signs or symptoms suggestive of SARS appear. Reported by: YS Leo, MBBS, Communicable Disease Center; M Chen, MBBS, BH Heng, MSc, CC Lee, MRCP, N Paton, MD, B Ang, M Med, P Choo, MBBS, SW Lim, Tan Tock Seng Hospital; AE Ling, MBBS, ML Ling, MBBS, BK Tay, MBBS, Singapore General Hospital; PA Tambyah, MBBS, YT Lim, FRCP, National Univ Hospital; G Gopalakrishna, MSc, S Ma, PhD, L James, M Med, PL Ooi, MSc, S Lim, MSc, KT Goh, MSc, SK Chew, MSc, CC Tan, FRCP, PhD, Ministry of Health, Singapore. Editorial Note:The experience with SARS in Singapore is analogous to that in Hong Kong, Vietnam, and Canada, where the first cases were associated with a large number of health-care--associated infections. During the early phase of the outbreak in Singapore, the original imported case and a nurse contact were associated with two large clusters. However, subsequent clustering was associated with cases that either had atypical clinical presentations masking their infections or were otherwise not rapidly identified because of lack of an initial history of direct contact with a known SARS case. Consequently, these patients became hidden reservoirs of infection on the wards of health-care facilities or in the community. SARS patients with chronic illnesses occurring concurrently with fever and/or pneumonia with a plausible diagnosis are the most challenging to the public health and health-care systems. This was the situation for Cases 3, 4, and 5 described in this report, who were retrospectively identified as SARS cases despite heightened clinical vigilance for new cases. Because of this spectrum of clinical presentations, MOH has adopted a strategy to quickly identify febrile or symptomatic persons with chronic illnesses or any recent health-care--facility contact as suspected cases for isolation. Super spreaders have been described with other diseases such as rubella, laryngeal tuberculosis, and Ebola (3). This phenomenon might be the result of a combination of host, environment, and virus interactions. A common feature of the super spreaders described in this report was nosocomial transmission, with hospitals serving as sources for disease amplification. This has implicated the adequacy of infection-control measures although the last super spreader also spread disease among his social contacts, and the super spreader reported from Hong Kong spread virus in Hotel M. Moreover, many secondary cases reported only limited contact with these patients. Additional data on the natural history of infection are needed to understand factors that might be associated with this phenomenon. Regardless of whether this phenomenon is the result of other transmission routes, inadequate infection-control measures, or more viral shedding by a patient, transmission of SARS virus is highly efficient in some circumstances. The preliminary reports from Hong Kong and Vietnam described transmission after direct contact with probable cases. Although this appears to be true for the majority of cases, initial contact tracing and isolation measures based on this assumption were too narrowly defined to prevent secondary transmission in Singapore. On the basis of descriptions of transmission resulting from undefined or limited contact (e.g., in corridors, elevators, and taxis and to visitors to the same inpatient ward) coupled with recent reports of prolonged environmental contamination, a much more expanded policy for contact tracing and home quarantine has been instituted in Singapore. The national prevention and control strategy for SARS focuses on 1) eliminating nosocomial transmission through substantially enhanced infection-control practices, 2) preventing additional importations of infection through health screening and travel advisories at the airport and seaports, and 3) stopping community transmission through education, contact tracing, and quarantine measures. Indicators of the effectiveness of this approach include the lack of nosocomial transmission on SARS-specific wards in TTSH/Communicable Disease Center since the designation of those wards on March 22 and in the remainder of the hospitals since April 17, and no further transmission of infection from imported cases. References
* Persons who directly infected >10 other persons. † This report is being published concurrently in the Weekly Epidemiological Record.
Figure 1
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 5/8/2003 |
|||||||||
This page last reviewed 5/8/2003
|