 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
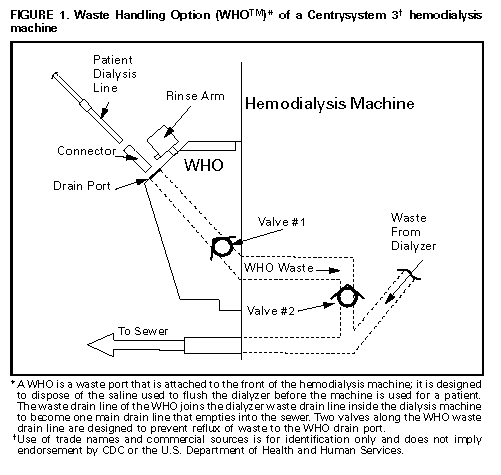
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Outbreaks of Gram-Negative Bacterial Bloodstream Infections Traced to Probable Contamination of Hemodialysis Machines -- Canada, 1995 United States, 1997; and Israel, 1997During 1996, approximately 236,000 persons received hemodialysis in the United States; of these, an estimated 183,000 (78%) received chronic hemodialysis (1). Patients who receive chronic hemodialysis are at increased risk for bloodstream infections (BSIs) because of the need for repeated vascular access. Reported BSI rates for hemodialysis patients have ranged from 8.4 to 16.8 episodes per 100 patient-years (2), and BSI has been identified as the cause of death in 6%-18% of hemodialysis patients (2). Outbreaks of BSIs in hemodialysis units usually have been caused by inadequate disinfection of 1) water treatment or distribution systems (3,4) and 2) reprocessed dialyzers (5-8). This report summarizes the investigations of three clusters of gram-negative bacterial BSIs at hemodialysis centers in Canada, the United States, and Israel. The findings indicate that all three outbreaks probably resulted from contamination of the waste drain ports in the same model of hemodialysis machine. Canada From June 17 through November 15, 1995, nine adult patients at an ambulatory hemodialysis center in Montreal, Canada, had Enterobacter cloacae BSIs. All patients at the hemodialysis center were dialyzed on COBE {Registered} Centrysystem 3 * (CS3, GAMBRO {Registered} Healthcare {TM}, Lakewood, Colorado) hemodialysis machines. Each CS3 had a Centry {Registered} Waste Handling Option (WHO {TM}), which is a waste port designed to dispose of the saline used to flush a dialyzer before the machine is used for a patient Figure_1. The WHO waste drain line employs two one-way valves to prevent drain line waste from refluxing into the WHO. The investigation indicated that at least one of the two one-way valves in the WHO waste drain lines of seven of 11 machines were incompetent, ** potentially allowing drain backflow and contamination of dialysis lines in contact with the WHO port. An epidemiologic investigation demonstrated that case-patients (i.e., the nine patients at the hemodialysis center who had Enterobacter cloacae BSIs) were more likely than control-patients to have received dialysis on a machine that had at least one incompetent valve on the WHO waste drain line (all seven case-dialysis sessions versus 145 {53%} of 272 control-dialysis sessions; odds ratio: undefined; p=0.02). Case- and control-patients were otherwise similar in demographic characteristics, underlying renal disease, type of vascular access, and dialyzer type. Enterobacter cloacae isolated from all nine infected patients and from the WHOs of 10 of 11 dialysis machines were identical when examined by pulsed field-gel electrophoresis (PFGE). United States From December 5, 1996, through January 25, 1997, a total of 10 adult patients at an ambulatory hemodialysis center in Maryland had gram-negative bacterial BSIs. Six BSIs were caused by Enterobacter cloacae, four by Pseudomonas aeruginosa, and two by Escherichia coli; two were polymicrobial BSIs. All patients at the hemodialysis center were dialyzed on CS3 hemodialysis machines that had WHOs. Results of a cohort study of all patients receiving dialysis at the center during the 2-month epidemic period indicated that the risk for gram-negative BSI was associated with exposure to any of three particular dialysis machines (seven BSIs in 20 patients who were exposed to one or more of the three machines versus three BSIs in 64 patients who were exposed to the other machines; relative risk=7.5; 95% confidence interval=2.1-26.2). Incompetent valves on WHO waste drain lines were present in eight of 26 dialysis machines and in two of the three implicated machines. Enterobacter cloacae was recovered from the WHOs of 14 of 26 machines, and P. aeruginosa was recovered from seven of 26. PFGE patterns of available Enterobacter cloacae isolates from the dialysis machines and from three patients were identical; none of the P. aeruginosa isolates obtained from patients were available for PFGE testing. Israel From February 9 through September 19, 1997, eight adult patients at an ambulatory hemodialysis center in Jerusalem, Israel, had gram-negative bacterial BSIs. BSIs in four patients were caused by Escherichia coli, three by P. aeruginosa, two by Enterobacter cloacae, and one by Stenotrophomonas maltophilia; two patients had polymicrobial BSIs. All patients at the hemodialysis center were dialyzed on CS3 hemodialysis machines that had WHOs. All eight patients who had BSIs had been dialyzed on three of 13 dialysis machines. Backflow was observed in the WHOs of the three implicated dialysis machines, and cultures obtained from the WHOs of six of 13 machines were positive for gram-negative organisms. Five of the eight patients, including all four with Escherichia coli BSIs, had been dialyzed on one machine that subsequently was culture-positive for Escherichia coli and P. aeruginosa. Both patients with Enterobacter cloacae BSIs had been dialyzed on a second machine that was culture-positive for Enterobacter cloacae and P. aeruginosa. Escherichia coli isolates obtained from three patients and the WHO of the implicated machine were identical by PFGE. Follow-Up Investigation Daily quality-control testing of WHOs as specified by the manufacturer had not been performed at any of the three hemodialysis centers. The manufacturer specifies that preventive maintenance of the valves in the WHO waste drain line includes replacement of the two valves after every 2000 hours of use. However, personnel at the three hemodialysis centers were aware of the need to change only one valve in the WHO waste drain line, and personnel at two centers did not know a second WHO valve existed; schematic diagrams provided by the manufacturer to these two hemodialysis centers identified only one of the two valves. At one center, experimentally bending and twisting the main drain line of a machine that had incompetent valves in the WHO waste drain line demonstrated the ease with which backflow can occur in the WHO. In one hemodialysis center, the outbreak was controlled after high-level WHO disinfection (i.e., disinfecting dialysis machines with formaldehyde on two occasions and increasing the dwell time for routine weekly machine disinfection). In the other two centers, the outbreaks were terminated by discontinuing use of the WHO. All three hemodialysis centers discontinued using the WHOs. In June 1997, GAMBRO Healthcare sent a Medical Device Safety Alert letter to all hemodialysis centers of record that use the CS3. This letter informed users of the need to ensure proper functioning of the WHO and outlined procedures for proper disinfection and maintenance of the equipment. Reported by: C Frenette, MD, M Delorme, Hopital Charles LeMoyne, Quebec; J Hockin, Health Canada, Ottawa, Ontario, Canada. FG Grillo, MD, T Killar, SJ Boyer, Maryland; DM Dwyer, MD, State Epidemiologist, Maryland Dept of Health & Mental Hygiene. C Block, MBBCh, R Backenroth, MD, M Shapiro, MD, Hadassah Univ Hospital, Jerusalem; B Lev, MD, Associate Director General, Israel Ministry of Health. Hospital Infections Program, National Center for Infectious Diseases; and EIS Officers, CDC. Editorial NoteEditorial Note: Bacterial BSI is a potentially severe complication associated with hemodialysis vascular access. In the United States, complications associated with vascular access represent one of the most common sources of morbidity among patients undergoing end-stage renal dialysis, with associated costs exceeding an estimated $1 billion per year (9). This report links three outbreaks of gram-negative bacterial BSIs to a unique design feature of the CS3 hemodialysis machine. The results of these outbreak investigations demonstrated that the WHO, if not properly maintained and disinfected, may be a source of bacterial contamination leading to BSIs in hemodialysis patients. Because waste backflow can occur with incompetent valves and WHO contamination can occur easily, the design of the WHO creates a mechanism for possible cross-contamination of the patient dialysis line. In addition to the problems associated with the WHO feature, insufficient training of hemodialysis personnel about the design and proper handling and maintenance of WHOs might contribute to transmission of BSIs to hemodialysis patients. In June 1996, GAMBRO Healthcare and CDC surveyed 595 U.S. dialysis centers that use CS3 machines to characterize the methods used to clean and disinfect the dialysis machines and to characterize quality-control procedures (GAMBRO Healthcare and CDC, unpublished data). The survey indicated that personnel at most (87%) of the responding dialysis centers reported weekly disinfection of their dialysis machines as specified by COBE guidelines, although most (62%) were not disinfecting dialysate and bicarbonate sampling ports as often as recommended. Of the 290 centers that reported using the WHO, only 42 (14%) performed the recommended daily quality-control assessment of the WHO valves to determine whether drain reflux was occurring. Of the 137 centers responding to the question "If fluid can be aspirated from the WHO, what is done?," 112 (82%) indicated the need for replacing WHO valves or taking the machine off-line for servicing. This report underscores the importance of surveillance and infection control in the ambulatory health-care setting. The detection of these outbreaks and identification of the likely cause was aided by the brief time-frame during which multiple infections were identified. The limited availability of data about infection rates in ambulatory dialysis centers impedes the identification of small or prolonged low-level outbreaks. Because of the lack of such data, inappropriate infection-control or maintenance practices that were identified in the GAMBRO Healthcare/CDC survey could not be linked to adverse patient outcomes at the dialysis centers surveyed. Outbreaks of gram-negative bacterial BSIs in hemodialysis patients that appear to be associated with use of the WHO should be reported to state health departments and to CDC's Hospital Infections Program, National Center for Infectious Diseases; telephone (404) 639-6413. References
* Use of trade names and commercial sources is for identification only and does not imply endorsement by CDC or the U.S. Department of Health and Human Services. ** The manufacturer recommends daily testing of the competency of WHO valves by filling a 30 cc syringe with water, injecting the
contents into the WHO drain port, and attempting to draw back
fluid
from the WHO. Competent valves should prevent backflow. Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 10/05/98 |
|||||||||
This page last reviewed 5/2/01
|
{kind=link}