 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
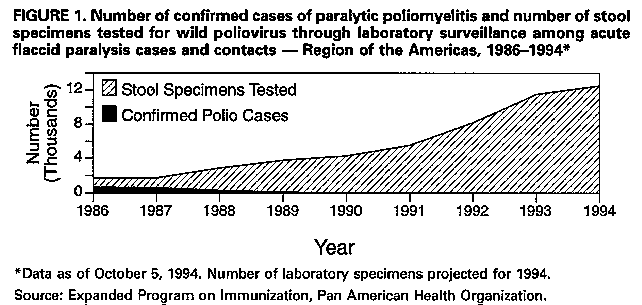
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. International Notes Certification of Poliomyelitis Eradication -- the Americas, 1994In May 1985, the Pan American Health Organization (PAHO) proposed the goal of interruption of wild poliovirus transmission in the Western Hemisphere by 1990 (1). This proposal was endorsed by all member governments and was supported by several agencies and organizations, including Rotary International, the U.S. Agency for International Development, the United Nations Children's Fund, the Inter-American Development Bank, and the Canadian Public Health Association. On August 20, 1994, PAHO reported that 3 years had passed since the occurrence of the last case of poliomyelitis associated with wild poliovirus isolation in the Americas (Peru, August 1991) (2). This report summarizes the steps to certify eradication of polio in the Americas. In 1990, PAHO established an independent International Commission for the Certification of Poliomyelitis Eradication in the Americas (ICCPE) (3) to oversee the regional polio eradication efforts and to determine when the goal has been achieved. The ICCPE required three criteria before the Region of the Americas could be certified as polio-free: 1) high (i.e., more than 80%) levels of vaccination coverage with poliovirus vaccine, 2) adequate surveillance for polio cases (as defined by a series of specific indicators recommended by the ICCPE), and 3) at least 3 years without any confirmed polio cases (4). In early 1994, the 38 member countries formed 25 independent national certification commissions and one multinational commission for the English-speaking Caribbean countries to evaluate national data and to recommend to the ICCPE whether poliovirus transmission had been interrupted in their respective countries. Information reviewed by the National Certification Commissions included 1) trends in vaccination coverage; 2) national surveillance data obtained from an extensive regionwide surveillance system with more than 20,000 health units that report weekly on the presence or absence of cases of acute flaccid paralysis (suspected polio cases); and 3) laboratory results from the testing of stool specimens obtained from persons with suspected polio and their contacts for the presence of wild poliovirus. In 1993, regional vaccination coverage among children with at least three doses of oral poliovirus vaccine was 87%; 33 of 38 countries had achieved and maintained coverage of more than 80%. Routine vaccination has been supplemented by annual national immunization days *. Since August 21, 1991 (when the last confirmed case was reported), approximately 6000 acute flaccid paralysis cases have been investigated; however, none of these cases were confirmed as paralytic polio resulting from wild poliovirus. In addition, approximately 25,000 stool specimens obtained from these patients and their contacts were negative for wild poliovirus (Figure_1). Finally, key surveillance indicators have been at acceptable levels in all countries during the past 3 years. Based on review of these data, all 26 national or multinational certification commissions recommended that their countries be certified as polio-free. Based on recommendations of the national certification committees and after review of surveillance and laboratory data, on September 29, 1994, the ICCPE announced that wild poliovirus transmission has been interrupted in the Americas. Reported by: Expanded Program on Immunization, Pan American Health Organization, Washington, DC. Editorial NoteEditorial Note: The certification of the interruption of wild poliovirus transmission in the Americas is an important achievement in the global effort to eradicate poliovirus. In addition to successful vaccination strategies, other factors that contributed to this achievement included 1) the high level of political commitment of the member governments; 2) substantial community participation; and 3) strong collaboration among participating agencies and organizations through interagency coordinating committees. Although poliovirus transmission has been interrupted in the Americas, transmission of wild poliovirus continues in other parts of the world and creates an ongoing risk for the importation of wild poliovirus into the Americas (5). If importations occur, polio outbreaks may develop, especially in localities with low vaccination coverage and poor sanitation (6-8). As a result, the Region of the Americas must maintain high levels of vaccination coverage. Ongoing surveillance for acute flaccid paralysis cases and for the presence of wild poliovirus must be maintained. International communication and collaboration will continue to be necessary for the rapid detection of importations of wild poliovirus and timely implementation of control efforts. Only the global eradication of polio will ensure that the Region of the Americas remains polio-free. References
* Mass campaigns over a short period (days to weeks) in which two doses of OPV are administered to all children in the target group, regardless of prior vaccination history, with an interval of 4-6 weeks between doses. Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 09/19/98 |
|||||||||
This page last reviewed 5/2/01
|
{kind=link}