|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
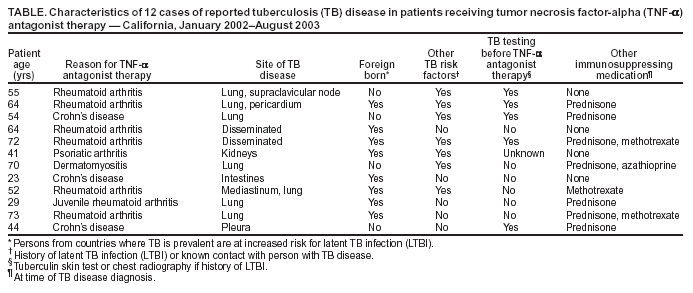
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Tuberculosis Associated with Blocking Agents Against Tumor Necrosis Factor-Alpha --- California, 2002--2003The Food and Drug Administration (FDA) has determined that tuberculosis (TB) disease is a potential adverse reaction from treatment with the tumor necrosis factor-alpha (TNF-α) antagonists infliximab (Remicade®), etanercept (Enbrel®), and adalimumab (Humira®)*; the three products are labeled accordingly (1,2). These products work by blocking TNF-α, an inflammatory cytokine, and are approved for treating rheumatoid arthritis and other selected autoimmune diseases. TNF-α is associated with the immunology and pathophysiology of certain infectious diseases, notably TB; blocking TNF-α can allow TB disease to emerge from latent Mycobacterium tuberculosis infection. In 2002, a California county health department reported three cases of TB disease occurring in association with infliximab therapy. This report summarizes those cases and nine subsequently reported cases and provides interim recommendations for TB prevention and management in recipients of these blocking agents. Health-care providers should take steps to prevent TB in immunocompromised patients and remain vigilant for TB as a cause of unexplained febrile illness. Case ReportsCase 1. In January 2002, a U.S.-born man aged 55 years with rheumatoid arthritis had pulmonary TB disease diagnosed 17 months after starting infliximab therapy. In 1995, he had a positive tuberculin skin test (TST) and reportedly took isoniazid for 12 months; however, his adherence to therapy was questionable. During September 2000--January 2002, he received 13 infusions of infliximab, and his arthritic symptoms decreased. However, in January he had fever and weight loss. Four weeks later, a supraclavicular lymph node became enlarged, and a chest radiograph revealed a right-upper-lobe lung cavity with a nodular infiltrate. M. tuberculosis was isolated from sputum and lymph node specimens, and his condition improved with anti-TB medications. In July 2002, he again lost weight. He had smoked cigarettes for many years and was found to have lung cancer; he died in November 2002. Case 2. A woman aged 64 years with rheumatoid arthritis had pulmonary and pericardial TB disease diagnosed in June 2002. She had begun infliximab therapy in September 2001 and received 7 doses before onset of fever and weight loss in April 2002. Her chest radiograph revealed a large pericardial effusion and a right-upper-lobe lung infiltrate. M. tuberculosis resistant to isoniazid, rifampin, pyrazinamide, and ethambutol was isolated from sputum and pericardial fluid. The patient was born in the Philippines, where TB often is drug resistant (3). In 1999, she was exposed to a person with drug-susceptible TB in the United States and subsequently had two TSTs with negative results in 2000; however, she was taking prednisone for her arthritis at the time of the TSTs. After 12 months of therapy with second-line anti-TB medications, her medical condition has improved. Case 3. A U.S.-born woman aged 54 years was exposed to contagious TB in 1996; she had a positive TST result during the contact investigation but was not treated for latent TB infection (LTBI). The patient has Crohn's disease and received infliximab in February 2001 and June 2002. Two weeks after her second infusion, but 16 months after her first infusion, she sought care for cough, fever, and abdominal pain. Her chest radiograph revealed upper-lobe lung nodules with a pleural effusion, and sputum specimens yielded M. tuberculosis. She started standard, four-drug anti-TB therapy but experienced gastrointestinal intolerance. Isoniazid was discontinued, and she was free of TB disease after treatment with rifampin, pyrazinamide, and ethambutol. Additional ReportsIn 2003, the state of California Department of Health Services asked local jurisdictions to report TB cases associated with TNF-α antagonists since January 2002. As of September 2003, nine additional reports had been received, for a total of 12 cases diagnosed during January 2002--August 2003 (Table). The median patient age was 54.5 years (range: 23 to 73 years), and eight (67%) of the patients were female. Eleven of the patients had TB disease after receiving infliximab. One patient had TB disease while receiving chronic etanercept therapy. Eleven of the patients had at least one risk factor for LTBI (e.g., born in countries where TB is prevalent or contact with a person with TB disease). Eight were taking other immunosuppressive therapies at the time of their TB diagnoses. Three patients underwent a medical history for TB risk factors before beginning therapy with a TNF-α antagonist. In addition to the patient in case 1, a second patient died (from cardiomyopathy) while being treated for TB disease. Reported by: P Costamagna, K Furst, MD, K Tully, San Joaquin County Public Health Svcs; J Landis, Santa Cruz County Health Svcs; K Moser, MD, San Diego County Dept of Health; L Quach, J Kwak, County of Orange Health Care Agency; H Calvet, MD, B Lindsey, Long Beach City Dept of Health and Human Svcs; J Flood, MD, California Dept of Health Svcs. M Braun, MD, Center for Biologics Evaluation and Research; J Siegel, MD, Center for Drug Evaluation and Research, Food and Drug Administration. K Winthrop, MD, J Jereb, MD, Z Taylor, MD, M Iademarco, MD, K Castro, MD, Div of TB Elimination, National Center for HIV, STD, and TB Prevention, CDC. Editorial Note:As of January 2004, FDA's adverse-event reporting system had received several hundred reports, mostly from outside the United States, of TB disease in patients who received TNF-α antagonists. Manufacturers of these products are required to report known cases, but reporting is voluntary for others. The majority of the cases probably represent progression of LTBI to TB disease, although the contribution of newly acquired M. tuberculosis infection to the total number of reports is unknown (1). Reports have included atypical presentations, extrapulmonary and disseminated disease, and deaths (1,4,5). In California, after the initial three reports, nine additional cases of TB disease were reported during January 2002--August 2003 in patients taking TNF-α antagonists. Although reporting of TB cases is mandatory in California, reporting the association with TNF-α antagonists was voluntary, and an underestimate might have resulted. Eight of the 12 patients in California were born in countries where TB is prevalent. In certain instances, physicians had not screened for risk factors for M. tuberculosis infection or tested their patients for infection before beginning therapy with TNF-α antagonists. In other instances, testing was performed, but LTBI was not diagnosed, possibly because of cutaneous anergy. Many patients who receive TNF-α antagonists already are receiving other immunosuppressive therapies, and certain conditions such as rheumatoid arthritis also can decrease sensitivity to tuberculin; therefore, TST results at the time of initiating TNF-α antagonist therapy might be falsely negative. Some experts advocate treating for presumed LTBI when a candidate for TNF-α antagonists has risk factors for M. tuberculosis infection but a negative TST result (4,5). TNF-α, an inflammatory cytokine expressed by activated macrophages, T-cells, and other immune cells, plays a crucial role in the host response against M. tuberculosis and other intracellular pathogens. Infliximab and adalimumab are monoclonal antibodies; etanercept is a dimeric soluble form of the TNF-α receptor. All three products are approved for the treatment of patients with rheumatoid arthritis. Infliximab also is approved for Crohn's disease, and etanercept is approved for specific other arthritides and for psoriasis. Use of these agents has been associated with other life-threatening infectious diseases besides TB, including candidiasis, histoplasmosis, aspergillosis, and listeriosis (1). TNF-α antagonists often are used in conjunction with other immunosuppressive therapies, particularly glucocorticoids and methotrexate. Whether the increased rates of TB or other infectious diseases are caused by interactions among these therapies is unknown. Diagnosing LTBI in candidates for TNF-α antagonist therapy is challenging (Box). For patients who undergo treatment for LTBI, the optimal time for starting TNF-α antagonist therapy is undetermined. Some experts advocate postponing therapy until LTBI treatment is complete. However, this delay might be impractical (4,6). The risk for TB relapse in patients previously cured of TB disease and subsequently treated with TNF-α antagonists is unknown. If active TB disease develops during TNF-α antagonist therapy, the TNF-α antagonist should be discontinued, at least until the anti-TB regimen has been started and the patient's condition has improved. The optimal time for resuming TNF-α antagonist therapy is undetermined. Outcomes with other immunosuppressive agents during the treatment of TB disease have been variable. Use of glucocorticosteroids during the treatment of TB disease is considered safe (7), and studies of TB disease in organ transplant recipients suggest that survival is not decreased by the use of cyclosporine or azathioprine (8). Etanercept, administered in a phase-1 clinical trial along with a standard initial anti-TB regimen, did not delay the resolution of TB disease markers in a group of patients coinfected with human immunodeficiency virus in comparison with historical controls; adverse effects were not detected (9). However, use of anti--T-cell agents in transplant recipients with TB disease is associated with increased mortality; whether this increased mortality is because of the suppression of immune response or the dysfunction of the transplanted organ is unclear (8). Practitioners who prescribe TNF-α antagonists should educate their patients about the symptoms of TB disease, with added emphasis on extrapulmonary symptoms, which can include fever, malaise, or development of a mass. A patient with symptoms should undergo diagnostic testing for TB. In addition to following local reporting requirements, health-care providers should report TB cases associated with TNF-α antagonists to FDA's Medwatch system (available at http://www.fda.gov/medwatch). Ongoing clinical trials are using both approved and experimental TNF-α antagonists in the treatment of additional conditions (4). Novel therapies that inhibit other related inflammatory cytokines are under development. As the use of these blocking agents expands, associated cases of TB might increase. Vigilance for TB in association with these agents is critical to early recognition and successful treatment. References
* Respectively, Centocor, Malvern, Pennsylvania; Immunex Corporation, Thousand Oaks, California; and Abbott Laboratories, Abbott Park, Illinois. Table
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 8/5/2004 |
|||||||||
This page last reviewed 8/5/2004
|